Current Research Findings
and Information
The best-known effect of smoking is that it causes
cancer. Smoking can also aggravate many problems that people with diabetes
already face, such as heart and blood vessel disease.
1. Smoking cuts the amount of oxygen reaching tissues. The decrease in
oxygen can lead to a heart attack, stroke, miscarriage, or stillbirth.
2. Smoking increases your cholesterol levels and the levels of some other
fats in your blood, raising your risk of a heart attack.
3. Smoking damages and constricts the blood vessels. This damage can worsen
foot ulcers and lead to blood vessel disease and leg and foot infections.
4. Smokers with diabetes are more likely to get nerve damage and kidney
disease.
5. Smokers get colds and respiratory infections easier.
6. Smoking increases your risk for limited joint mobility.
7. Smoking can cause cancer of the mouth, throat, lung, and bladder.
8. People with diabetes who smoke are three times as likely to die of
cardiovascular disease as are other people with diabetes.
9. Smoking increases your blood pressure.
10. Smoking raises your blood sugar level, making it harder to control your
diabetes.
11. Smoking can cause impotence.
Vitamin
C for Smokers - A Long Shot
A study showing that injecting chronic smokers
with vitamin C helped their arteries widen made headlines when it was published
in the July 1 Circulation. But smokers shouldn't think they can pop pills to
avoid heart disease.
Cigarette smoke contains chemicals called
free radicals, which initiate a chain of artery- damaging events. They make LDL
("bad" cholesterol) stickier and more likely to cause atherosclerosis
(clogged arteries). Vitamin C is an antioxidant—a substance that mops up
free radicals before they wreak havoc.
In this small all-male study, 10 nonsmokers
and 10 long-time smokers (a pack a day for more than 20 years) were first given
shots of a chemical that relaxes the lining of the arteries. The result in
nonsmokers was wider arteries, but as expected, the smokers' arteries didn't respond
well. Then all the men were injected with vitamin C. When researchers tried the
chemical again, the smokers' arteries widened much more. But is this a
"cure" for smoking-induced atherosclerosis?
"Not by a long shot," says
HealthNews associate editor Harry Greene, MD. About
one gram of vitamin C was injected directly into the men's arteries; you'd have
to swallow a lot of pills to get this amount into your bloodstream, and daily
injections aren't very appealing. Also, the widening effect was probably
temporary, according to the researchers. And the study only looked at the arm
arteries; coronary arteries might react differently.
Increasing your vitamin C intake probably
won't help. A large study published in 1993 by Eric Rimm, an assistant
professor of epidemiology at the Harvard School of Public Health, found no
evidence that high intakes of vitamin C, from pills or food, could reduce
smokers' risk of heart disease. His advice: "The best thing for smokers to
do is quit."
Courtesy of HealthNews from the Publishers of the
Just Trying to Quit Smoking can Add Years to Life
SOURCE:
Annals of Internal Medicine, 2005;142:233-239
Smokers
assigned to a quit-smoking program, regardless of whether or not
they
actually quit, had lower death rates than those assigned to usual care,
according to
a new study.
Researchers
for the Lung Health Study evaluated 5,887 middle-aged smokers
with mild
lung disease who were randomly assigned to either a quit-smoking
program
(behavior modification and nicotine gum) or usual care. Study
participants
were followed an average of 14.5 years.
Results show
while only 21.7 percent of those in the quit-smoking program
had actually
quit smoking after five years (compared with 5.7 percent who
received the
usual care), even the non-quitters in the quit-smoking program
had a
15-percent lower death rate than smokers who received usual care.
So why did
those in the quit-smoking program who remained smokers still reap
some health
benefits?
Study author
John E. Connett, Ph.D., professor of biostatistcs at the
University
of Minnesota School of Public Health in Minneapolis, says,
"People
quit, restarted, and quit again. However, quitting had such a
statistically
large impact on the overall population that even though many
people quit
and started smoking again, as long as they were smoke free for
periods of
time, they had better outcomes than those who continued to
smoke."
As expected,
those who had quit smoking altogether during the study had
death rates
that were 46-percent lower than those who continued to smoke.
Smoking Makes Root Canals Likelier
People
Who Smoke at Least 12 Years Most Vulnerable
Courtesy of Miranda Hitti
New research shows
that smokers are more likely than nonsmokers to get root canals.
Root canals are
done when a tooth's dental pulp -- which includes nerves, blood vessels, and
connective tissue -- becomes infected and inflamed. The infected tissue is
removed, and then the hollow area is cleansed and filled to prevent the
infection's return.
Elizabeth Krall
Kaye, PhD, MPH, and colleagues reported their findings in New York, at a media
teleconference organized by the American Medical Association and American
Dental Association.
"Our study
has shown that men have almost twice the risk of having root canal treatments
if they smoke cigarettes, compared to men who never smoke," Kaye said, in
the teleconference.
Kaye is a
professor in the department of health policy and health services research at
Boston University's Goldman School of Dental Medicine.
About the Study
Kaye's team got
data from a study of 811 men who were followed for up to 28 years. The study
started in the late 1960s and early 1970s. Back then, the men were about 48
years old, on average. The men were mostly middle-class whites.
Every three
years, the men got their teeth examined and had dental X-rays taken at the
study site. The men also reported their smoking habits.
A total of 230
men had never smoked. Another 440 men were former smokers. Most of the smokers
smoked cigarettes. Few smoked pipes or cigars.
The researchers
checked the X-rays to see if root canals had been done. They spotted 998 teeth
that had root canals done on them. Those teeth belonged to 385 men, so many men
got more than one root canal.
Reduce the Odds of Root Canal
Among current
smokers, those who had smoked for more than 12 years were most likely to have a
root canal. Current smokers who had smoked for fewer years had a lower risk,
but they were still more likely than nonsmokers to have root canals.
Pipes and
cigars weren't linked to high odds of getting root canals. But there wasn't
much data on those smokers, Kaye's team notes.
Quitting cigarettes
-- and staying smoke-free -- helped, the study shows.
"There is
good news from this study for people who do smoke, and that is that if you
quit, your risk of root canal treatment will go down," Kaye says. She
notes that men who quit cigarettes for nine or more years were about as likely
as lifelong nonsmokers to get root canals.
Dentists' Role
All dentists
should ask their patients if they smoke and want to quit, Kaye notes.
"Dentists
can provide the nicotine patch and other types of cessation products, and they
can refer them to smoking cessation clinics and programs," she says.
"I think it should be a part of every dentist's program."
The X-rays
don't show why cigarette smokers were more likely than nonsmokers to get root
canals. "We couldn't in this study determine what the biological
mechanisms might be," Kaye says.
She and her
colleagues describe several possibilities in their report:
·
Smoking makes it harder to fend off
infections.
·
Smoking increases inflammation.
·
Smoking damages the circulation system
and lowers oxygen levels.
Kaye also
points out that the "dose-response" findings of this study strengthen
the case that smoking is a cause of dental disease. The men who smoked the most
had the highest number of root canals, and the nonsmokers and those that had
quit the longest had the least.
The findings
probably apply to women, Kaye says. "Perhaps it might be harder to detect,
because at least historically, women haven't smoked as long or as much per day
as men have, but I think the risk would still be there."
Lose Weight and Quit Smoking With
New Drug
Rimonabant Fights Munchies, Urge to Smoke
Lose weight and
quit smoking? A new drug promises to help people do just that.
The drug is called
rimonabant. And no, you can't get it -- yet. But early data from advanced
clinical trials may indicate you may see it before too long. Its planned brand
name -- pending FDA approval -- is Acomplia.
It's already
picked up a nickname: the munchies drug. That's because rimonabant acts like
marijuana in reverse, cutting appetite and curbing the craving for nicotine. In
two large-scale clinical trials, the drug has helped people with weight loss
and smoking cessation.
Researchers and
officials from drug maker Sanofi-Synthelabo today held a press conference to
discuss the findings.
"Those who
stay on drug for a year show remarkable weight loss: 17 pounds," said Jean
Pierre Despres, PhD, professor of food and nutrition sciences at Laval
University, in Montreal. "And we saw a remarkable reduction in waist
circumference of 8 centimeters or [3 inches]."
"Rimonabant
... roughly doubled the odds of quitting smoking," said Robert Anthenelli,
MD, associate professor of psychiatry at the University of Cincinnati College
of Medicine. "We also found remarkably reduced postcessation weight gain:
a 77% reduction versus placebo. ... These dual effects on smoking cessation and
reduced weight gain make rimonabant a promising agent for treating tobacco
dependence."
Weight Loss
Where It Counts
The weight-loss
study enrolled more than 1,000 moderately obese men and women whose cholesterol
and blood-fat levels put them at high risk of diabetes. Half of them had what
is known as the metabolic syndrome, a combination of abdominal fat, high blood
pressure, high blood-fat levels, low levels of "good" HDL
cholesterol, and high blood-sugar levels.
After a year on
a diet that restricted daily calories by 600, more than one in four study
participants who got inactive placebo pills lost more than 5% of their body
weight. Only one in 10 lost more than 10% of their body weight. But nearly
three of four participants who got 20 mg doses of Acomplia lost at least 5% of
their body weight -- and nearly half lost more than 10%.
That's impressive
weight loss for any clinical trial. But Despres says that people who took
Acomplia lost the most dangerous pounds -- abdominal fat. Half of those who had
metabolic syndrome no longer had the condition after treatment with the
20-milligram dose of Acomplia.
"I am very
impressed in the increase in [good] HDL cholesterol generated by this one-year
rimonabant therapy," Despres said. "The 20-milligram dose was able to
generate a 20% increase in HDL, accompanied by more than a 10% decrease in triglycerides
[blood fats]. Those who completed the full study had even more spectacular
results: a 25% increase in HDL."
Quit
Smoking, Gain Less Weight
A different
clinical trial tested whether rimonabant can help people quit smoking. The
10-week trial enrolled nearly 800 men and women. Before starting the study,
they smoked an average 23 cigarettes a day. Their goal: to quit smoking for at
least four weeks straight.
Among those who
completed the study, one in five people managed to quit smoking even though
they got only inactive placebo pills. But more than one in three people (36.2%)
who got 20-milligram doses of rimonabant were able to quit.
None of these
smokers was obese. But those who quit smoking while taking placebo pills gained
6.6 pounds. Those who got 20 milligrams of rimonabant gained only 1.5 pounds.
A one-year
continuation of the trial is underway in the U.S. and Europe.
Anti-Marijuana?
It's not
totally misleading to call rimonabant anti-marijuana. The medical name for
marijuana is cannabis. And scientists have recently discovered that the human
body makes marijuana-like molecules called cannabinoids. These molecules
regulate how the body uses and stores energy, as well as immune function. To do
this, they plug into receptor molecules on the outside of nerve cells, fat
cells, and immune cells.
Rimonabant is
the first of what promises to be a slew of new drugs that take advantage of
these findings. There are two kinds of cannabinoid receptors, known as CB-1 and
CB-2. The CB-1 receptors are found on nerve and fat cells. Rimonabant blocks
these CB-1 receptors.
Douglas A.
Greene, MD, Sanofi-Synthelabo vice president for regulatory affairs, says that
obese people and people with a craving for nicotine have an overactive
cannabinoid system. By partially blocking this system, rimonabant helps people
lose weight and quit smoking.
A Heart Drug
So is
rimonabant a weight-loss drug or a smoking-cessation drug? Greene says it's
both and neither. He prefers to think of it as a heart-health drug.
"This
compound is completely novel," he says. "It is the first in a class
of new medications that has effects on two major cardiovascular risk factors.
These are probably the two major preventable risk factors for heart disease:
smoking and obesity. This represents a major medical advance for patients at
risk of heart disease. This is an important medical therapy that will have a
major public health impact."
Stay tuned.
More detailed results from these and other studies will be announced next month
at a major medical meeting.
Courtesy of Daniel DeNoon.
Women quitting smoking
faster than men
Latest statistics compiled
by the US's Centers for Disease Control and Prevention have found that women
are quitting smoking in greater numbers as compared to men.
Data collected by the centre
has revealed that the percentage of women who smoke has dropped down below 20
percent. While in 2003, the number of women who smoked was a mere 19.2 percent,
the numbers of male smokers stood at 24.1 percent.
Experts however believe that
despite the dip in the national average from 22.5 percent in 2002 to 21.6
percent in 2003, the rate is not fast enough to reach the magic figure of 12
percent by 2010.
"It's wonderful that
it's trending down. But we still need to fight and keep our guard up about very
innovative and clever marketing by the tobacco industry," The New York
Daily News quoted Dr. Avi Barbasch, an oncologist on board the directors of the
American Cancer Society as saying.
The study further revealed
that Native American male population had 42 percent smokers, the Hispanic and
the Asian women had only 10 and seven percent smokers respectively.
"Passive"
tobacco inhalation increases risk by 30%
Courtesy of Richard N. Fogoros, M.D., a former professor of medicine, and
a longtime practitioner, researcher and author in the fields of cardiology and
cardiac electrophysiology.
In a study published in
Circulation on May 23, investigators report that the cardiovascular system of nonsmokers
is extremely sensitive to tobacco toxins inhaled during passive smoking. They
reached this conclusion by analyzing 29 studies that measured the risk of heart
disease in people who never smoked tobacco, but who were exposed to secondhand
smoke.
While secondhand smokers
only inhale about 1/100th the dose of smoke inhaled by the smokers themselves,
the effect of that secondhand smoke is large. Secondhand smokers have a risk of
coronary heart disease that is 30% higher than for nonsmokers who are not
exposed to secondhand smoke. In contrast, the risk for actual smokers is
increased by 80%. So, while the dose of smoke inhaled by passive smoking is 100
times smaller than for smokers, the increase in risk to the nonsmokers is much,
much greater than that.
Indeed, their excess risk is
almost 40% as high as the excess risk to the smokers themselves.
The investigators further
listed the effects that secondhand smoke have been
shown to have on the cardiovascular system that can lead to an increase in cardiac
disease. These include: making platelets stickier, causing inflammation,
reducing HDL cholesterol levels, increasing LDL cholesterol levels, and
increasing insulin resistance. Some of these effects can be measured after just
a few minutes of exposure to secondhand smoke.
The accumulating and
disturbing evidence against secondhand smoke is enough to make even DrRich, an
ardent supporter of individual freedoms, hope for even more restrictions on
smoking in public places.
Taking a Look Inside
They say a
picture is worth a thousand words and when it comes to quitting smoking, a
thousand words doesn’t seem like enough to describe what’s
happening to you body. Take a
look:
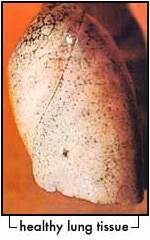


These
photographs are courtesy of Frederic W. Grannis Jr. M.D
Thanks for allowing them to be
used to help people
see the long term effects of
smoking.
Withdrawal - Physical
And Psychological
Symptoms
What Are the Physical
Symptoms of Nicotine Withdrawal?
The physical symptoms of nicotine
withdrawal vary from person to person, but may include any of the following: ·
- Increased appetite, especially for carbohydrates
and sweets
- Increased coughing and sputum production
- Sweating
- Fatigue
- Muscle aches and cramps
- Constipation or diarrhea
- Headache
- Hypersensitivity to stimuli
- Sleep disturbances
- Weight gain
- Nausea
What
Are The Psychological Symptoms of Nicotine Withdrawal?
Since tobacco users have a
habit of obtaining increased concentration and alertness from tobacco, they
sometimes experience feeling foggy, unfocused, unmotivated and forgetful for a
short time after they reduce or quit. Fortunately, these psychological symptoms
also pass their peak by the second or third day, then
drop rapidly. The psychological symptoms of nicotine withdrawal vary from
person to person, but may include any of the following:
- Irritability
- Restlessness
- Anxiety
- Increased aggressive thoughts and behavior
- Depression
- Decreased ability to tolerate stress or
disruption
- Decreased sexual drive
- Impaired work performance
Intense tobacco cravings Positive Physical, Psychological
and Environmental Symptoms of Nicotine Withdrawal?
Happily, there are many
positive psychological symptoms and physical effects to counterbalance the
negative effects of nicotine withdrawal. They include:
- Happiness about getting free from tobacco
- Happiness about being free of the self-nagging
and guilt about using tobacco products Improved abilities to smell and
taste
- Clothes, home, and car smell better every day
- None of the mess and dirt associated with
tobacco use
- Lowered blood pressure
- Lowered heart rate
- Improved circulation in the hands and feet
- Decreases in the carbon monoxide levels
- More oxygen to your brain and body
Generally feel better than
when you used tobacco products In addition, the natural cleansing systems in
your lungs begin to operate more effectively, and you experience a higher level
of health and well-being.
Quit Smoking and Save Your Skin!
Research from Nagoya City
University in Japan highlights the fact that smoking damages the skin's ability
to renew itself, diminishing collagen production by up to 40%. Collagen is the
skin's scaffolding, and without it the skin loses its elasticity and starts to
sag.
Professor Harryono Judodihardjo,
a leading cosmetic dermatologist and medical director of the Cellite Clinic in
"Cigarette smoke inhibits
this process as it contains more than 4,000 toxins. The smoke constricts the
blood vessels thereby reducing the amount of oxygen the skin receives."
The term "smoker's
face" entered the medical lexicon with an article written by Dr Douglas
Model for the British Medical Journal, in which he coined the expression.
The symptoms of "smoker's
face" include a number of distinct characteristics:
Prominent lines;
A gaunt appearance - sunken
cheeks;
Tough, dry, leathery skin;
A mottled, reddish; complexion caused
by inadequate oxygenation of the blood and, in some cases, a grey pallor due to
atrophy of the skin.
A study conducted by the Twin
Research Unit at
Scientists also believe that
smoking may impact adversely on DNA.
Professor Judodihardjo said,
"Evidence suggests that smoking may have a deleterious effect on DNA.
Damaged DNA in skin tissue can result in abnormal cell growth
which make be a factor in certain types of skin cancer.
"Smoking affects the skin's
ability to heal too. For this reason I don't offer certain treatments to heavy
smokers."
Smoking also adversely affects
the endocrinal system - the glands that secrete hormones - with the potential
for increasing the waist to hip ratio.
"Smokers may weigh less than
non-smokers, but the weight is distributed unevenly, which is why many smokers
have pot bellies and spindly legs," Professor Judodihardjo said.
The effects of smoking are
cumulative, so it's never too late to reap the benefits of quitting.
"My wholehearted advice to
smokers is to prevent further damage occurring to their skin, or any other part
of the body, by giving up tobacco immediately," Professor Judodihardjo
added.
"The sooner you quit, the
sooner the body can start to repair itself."
Urging Doctors to Do More to Stop Smoking...
A national smoking opponent urged doctors to do more to help smoking patients quit and stressed that workplaces need to be smoke-free for the health of employees.
Dr. Michael Fiore founder
and director of the University of Wisconsin Center for
Tobacco Research and Intervention since 1992, said one of his studies showed
doctors discussed tobacco use in only 21 percent of visits at 36 primary care
practices in
Doctors said in the study they didn't have enough time to
discuss tobacco use, patients didn't want to hear about it and they felt they
couldn't help their patients stop smoking.
"Even a brief encounter can make a difference,"
Fiore said. "A physician discussing tobacco use for three minutes can
increase abstinence rates."
Fiore spent the day in
Another study showed that smoking patients were more
satisfied with their health care when doctors asked about their smoking
addiction, Fiore said. "It's just the opposite of what physicians
think," he said. "Smokers expect us to bring up the topic."
Doctors are successful when they ask smokers about their
tobacco use, advise them to quit, assess their
willingness to quit, assist them in quitting and arrange follow-up, he said.
Doctors helping patients can increase their quit rates from 5 percent on their
own to 15 to 30 percent.
Fiore said smoking
workplaces hurt business and employees. He said customers expect a smoke-free
business today, and smoke-free workplaces increase quit rates among smoking
employees.
Smoking employees cost businesses more in lost productivity,
sick days and health-care costs, he said.
"Going smoke-free doesn't hurt business," Fiore
said. "Smoking hurts business."
Business leaders, including Dr. Robert Nesse of Franciscan
Skemp Healthcare, and Peter Hughes of Gundersen Lutheran, talked about making
hospitals and clinics smoke-free in the past several years and offering help
for smoking employees.
Nesse said he tells business leaders that smoking is related
to
Mayor John Medinger said
the smoke-free restaurant ordinance was a struggle but turned out to be a
success. Art Lotz, owner of Mr. D's Restaurant and Bakery, said his business
went smoke-free 10 months before the ordinance went into effect because more
people wanted a smoke-free dining experience.
"I wanted to eliminate the hassles," Lotz said.
"It has been a positive experience, and our business has held up. Smokers
came back, and we gained new customers. The ordinance has increased the dining
experience as a whole in
Fiore urged business leaders to support making all public
places and workplaces, including bars, smoke-free. Medinger said that would be
highly controversial, and the public would have to demand it. Fiore said
"People need to realize
the sky does not fall when you can't smoke in a restaurant or bar, or at
work," Fiore said. "You're protecting the public as well as
employees."
Smoking Habits May be Genetic
Whether a person starts smoking and how many cigarettes they
smoke a day may be largely determined by their genes, according to a new study.
Researchers found that having family members that smoke not
only increases the chance that young people will start smoking cigarettes, but
it also influences how many cigarettes they smoke per day and how addicted they
become to nicotine.
The large study of Dutch twins suggests that a combination of
shared genetics and environmental factors plays a major role in determining a
person's cigarette smoking habits.
But researchers say having a genetic predisposition for
nicotine addiction doesn't mean that someone will become addicted to tobacco or
unable to quit. They say smokers with a genetic predisposition can still quit
smoking, but they may find it harder to quit smoking than others.
The news comes as millions of Americans are trying to quit
smoking for at least one day as a part of today's annual Great American
Smokeout, sponsored by the American Cancer Society.
Hard to Quit Smoking? Blame Your Genes (Not Entirely)
In the study, published in The Pharmacogenomics Journal,
researchers looked into the link between genetics and smoking habits of 3,657
Dutch twin pairs. About half of the twins had never smoked.
They found both smoking initiation and number of cigarettes
smoked per day were strongly influenced by environmental and genetic factors.
For example, the study showed genetic factors explained 36% of
the variability in whether twins started smoking or not. Shared environmental
factors, such as exposure to smokers at school or in the neighborhood,
explained 56%.
In addition, researchers found shared genetic factors
explained 51% of the differences in how many cigarettes the participants
smoked, while shared environmental factors explained 30% of this difference.
Researchers say genes located on chromosomes 6 and 14 appear
to be involved in whether or not a person starts smoking, and a region on
chromosome 3 affects how many cigarettes are smoked a day.
But they say further research is needed to confirm these
results as well as determine whether genes might help explain why some people
have a harder time quitting smoking than others.
SOURCES: Vink, J. The
Pharmacogenomics Journal; vol 4: pp 274-282.
Can lung cancer be prevented?
Retinoid May Help Prevent Lung Cancer - Vitamin A Derivative May Lower
Risk Among Former Smokers
Quitting smoking is the single
biggest thing a person can do to reduce their risk of lung cancer, but now
researchers may have finally found a way to lower the risk for people who have
already quit their cigarette habit. A new study shows that daily treatment with
a retinoid drug may prevent lung cancer in former smokers.
Retinoids are natural and synthetic
compounds related to vitamin A (retinol) and retinoic acid (RA). Although they
have been found to help prevent head and neck cancers, until now retinoids have
not been shown to be effective in preventing lung cancer.
In fact, researchers say some studies
have shown that retinoids are of no benefit in reducing the risk of lung cancer
in current smokers. But this may be the first study that has shown a benefit in
targeting former smokers and reversing signs of precancerous lesions in lung
tissue.
Lung cancer is the leading cause of
cancer death in the U.S., and researchers say about 90% of all lung cancers
occur in people who smoke, which has made smoking cessation efforts a major
focus of lung cancer prevention efforts.
Although the risk of lung cancer
decreases in people who quit smoking, the risk still remains about twice as
high as those who have never smoked, for about 20 years after they quit. The
risk after 20 years lowers some but continues to remain high.
In the study, published in the Feb. 5
issue of the Journal of the National Cancer Institute, researchers looked at
the effects of two different types of retinoids on restoring the presence of a
substance called retinoic acid receptor beta (RAR-beta) in lung tissue from a
group of 226 former smokers. Loss of RAR-beta is considered a sign of
pre-cancerous tumors.
Researcher Jonathan M. Kurie, MD, of
the University of Texas M.D. Anderson Cancer Center in
Houston, and colleagues found a loss of RAR-beta in nearly 60% of the
participants at the start of the study.
But after three months of twice-daily
treatment with the retinoid known as 9-cisRA, there was a significant increase
in the presence of RAR-beta among those who received the retinoid compared with
the placebo. No benefit was found for the second type of retinoid tested.
Researchers say the study shows that
the benefits of retinoid treatment may differ among current vs. former smokers.
In an editorial that accompanies the
study, Jason S. Vourlekis, MD, and Eva Szabo, MD, of the National Cancer
Institute, say it remains to be seen how restoration of RAR-beta might
correlate to a reduction in risk of lung cancer, and more studies will be
needed to examine that issue.
SOURCE: Journal of the National Cancer Institute Jennifer
Warner WebMD Medical News
When will the cravings end?
Nicotine leaves the body, on the average, in 3-7 days (you can
speed up that process by drinking lots of water or fruit juice and by
exercising--with a doctor's supervision, ideally). That should take care of
most of the PHYSICAL cravings, which are generally the worst; but then there
are MENTAL/ EMOTIONAL/ BEHAVIORAL 'cravings' that you may have to deal with as
well. These urges to smoke can appear, occasionally and unexpectedly. The good
news is that, depending on how much work you're willing to do, or on how strong
your support network is, these unannounced cravings can usually be dismissed
quite easily and quickly. Many ex-smokers never again experience the urge to
smoke. The longer you have been quit the less frequent and less intense these
cravings are! It DOES get better with each and every passing day!
Information About Lung Cancer
Cigarette smoking is the single most important
preventable cause of lung cancer, accounting for 85% of all new cases of lung
cancer in
What is cancer?
Cancer is the development of
abnormal cells that grow out of control and form lumps called tumors. There are
two types of tumors - benign and malignant. Malignant tumors are the most
harmful and are often fatal. Benign tumors are more easily managed and
controlled through surgery and other therapies.
How does cancer
attack the lungs?
Cigarette smoke damages the lungs in
two ways:
Cigarette smoke inhibits and damages
the normal cleaning process by which the lungs get rid of foreign and harmful
particles. Smoke destroys an important cleansing layer in the lungs, which in
turn causes a build-up of mucus. The result is "smokers' cough," an
alternative method that the lungs take in attempting to clean themselves.
The harmful cancer-producing
particles in cigarette smoke are able to remain lodged in the mucus and develop
into cancer tumors.
Facts
Lung cancer will continue as the
leading cause of cancer death among Canadian women with an estimated 7,000
deaths in the year 2000. The number of new cases of women diagnosed with lung
cancer will increase to 8,400.8
The estimates for Canadian men who
will die of lung cancer in the year 2000 have risen to 10,700. The incidence of
new cases of lung cancer is estimated at 12,200.
In 1998, an estimated 17,100
Canadians died due to smoking-related lung cancer. Of the deaths caused by
smoking-related disease, lung cancer accounted for 31% of male deaths and 28%
of female deaths.
The risk of lung cancer increases
sharply the more you smoke and the longer you smoke.
Second-hand smoke is the primary
risk factor for contracting lung cancer among non-smokers. In
Screening and treatment for lung cancer
There are no tests or techniques
currently available that are effective in the early detection of lung cancer.
Routine screening for lung cancer is not recommended by any medical
organization. Treatment of non-small-cell lung cancer consists of various combinations
of surgical resection, chemotherapy and radiotherapy.
Currently, no single chemotherapy
regimen is recommended for routine use, although systemic chemotherapy can
produce partial responses and aid symptoms for short durations.
Reducing the risk of contracting lung
cancer
People who quit smoking greatly
reduce their risk of developing lung cancer compared with those who continue to
smoke.
In general, the longer you don't
smoke the greater the reduction in risk. The risk levels among long-term (10+
years) ex-smokers approaches those of non-smokers.
The Truth About "Light" Cigarettes: Questions and Answers
Many smokers choose "low-tar,"
"mild," or "light" cigarettes because they think that light
cigarettes may be less harmful to their health than "regular" or
"full-flavor" cigarettes.
After all, the smoke from light cigarettes feels
smoother and lighter on the throat and chest - so lights must be healthier than
regulars, right? Wrong.
The truth is that light cigarettes do not reduce the
health risks of smoking. The only way to reduce your risk, and the risk to
others around you, is to stop smoking completely.
What about the lower tar and nicotine numbers on light
cigarette packs and in ads for lights?
- These numbers come from smoking machines that "smoke"
every brand of cigarettes exactly the same way.
- These numbers do not really tell how much tar and nicotine a
particular smoker may get because people do not smoke cigarettes the same
way the machines do. And no two people smoke the same way.
How do light cigarettes trick the smoking machines?
- Tobacco companies designed light cigarettes with tiny pinholes on
the filters. These "filter vents" dilute cigarette smoke with
air when light cigarettes are "puffed" on by smoking machines,
causing the machines to measure artificially low tar and nicotine levels.
- Many smokers do not know that their cigarette filters have vent
holes. The filter vents are uncovered when cigarettes are smoked on
smoking machines. However, without realizing it and because they cannot
avoid it, many smokers block the tiny vent holes with their fingers or
lips -which basically turns the light cigarette into a regular cigarette.
- Because people, unlike machines, crave nicotine, they may inhale
more deeply; take larger, more rapid, or more frequent puffs; or smoke a
few extra cigarettes each day to get enough nicotine to satisfy their
craving. This is called "compensating," and it means that
smokers end up inhaling more tar, nicotine, and other harmful chemicals
than the machine-based numbers suggest.
- Cigarette makers can also make the paper wrapped around the tobacco
of light cigarettes burn faster so that the smoking machines get in fewer
puffs before the cigarettes burn down. The result is that the machine
measures less tar and nicotine in the smoke of the cigarette.
What is the scientific evidence about the health
effects of light cigarettes?
- The Federal Government's National Cancer
Institute (NCI) recently concluded that light cigarettes provide no
benefit to smokers' health.
- According to the NCI report, people who switch to
light cigarettes from regular cigarettes are likely to inhale the same
amount of hazardous chemicals, and they remain at high risk for developing
smoking-related cancers and other diseases.
- There is also no evidence that switching to light
or ultra-light cigarettes actually helps smokers quit.
What do tobacco companies say about the health effects
of light cigarettes?
- The tobacco industry's own documents show that
companies were well aware that smokers of light cigarettes compensate by
taking bigger puffs.
- Industry documents also show that the companies
were aware early on of the difference between machine-measured yields of
tar and nicotine and what the smoker actually inhales.
- The NCI report concluded that strategies used by
the tobacco industry to advertise and promote light cigarettes were
intended to reassure smokers and to prevent them from quitting, and to
lead consumers to perceive filtered and light cigarettes as safer
alternatives to regular cigarettes.
What is the bottom line for smokers who want to
protect their health?
- There is no such thing as a safe cigarette. The
only proven way to reduce your risk of smoking-related disease is to quit
smoking completely.
- Here's good news: Smokers who quit before age 50
cut their risk of dying in half over the next 15 years compared with
people who keep smoking.
·
Quitting also decreases your risk of lung cancer, heart
attacks, stroke, and chronic lung disease.
Courtesy
of the National Cancer
Institute
Secondhand Smoke Can Hide in Your
Home
Secondhand
tobacco smoke contaminants lurking in household dust and on furniture and other
surfaces can expose children to levels that are equivalent to several hours of
active smoking, says a study in the current issue of Tobacco Control.
The
study also says that making adults smoke outside doesn't fully protect children
from the harmful effects of tobacco smoke.
Researchers
compared 49 homes that included children between 2 and 12 months old.
Nonsmokers lived in 15 of the homes. Of the remaining 34 homes, 17 were occupied
by smokers who tried to protect their children by smoking outdoors. The other
17 homes were occupied by smokers who made no attempt to protect their children
from secondhand smoke.
Dust
and surface wipe samples were collected from the living room and the child's
bedroom in each of the homes. Urine and hair samples were taken from the
children. Nicotine monitors were placed in the living room and the child's
bedroom of each home.
Levels
of tobacco contaminants in the dust, air and surface samples of homes where
adults smoked outdoors were up to seven times higher than in homes of
nonsmokers. Tobacco contaminant levels in the homes of indoor smokers were up
to eight times higher than in the homes where adults went outside to smoke.
Infants
are particularly at risk from these indoor tobacco contaminants because they
spend most of their time indoors and are close to contaminated sources, the
study authors say.
Courtesy of HealthDayNews
Smoking Damages Reproductive Health
Report finds
pervasive effects on men, women and babies
A new British report says cigarette smoking causes
damage throughout a person's reproductive years and reduces the chance of
having healthy children.
The report advises anyone planning to have kids
to stamp out that cigarette butt once and for all.
The report, a comprehensive look at more
than two decades of studies on smoking and reproduction, concludes that the
damaging effects of smoking occur throughout a person's reproductive life, from
puberty to young adulthood and into middle age. This was true of both men and
women.
"There are so many aspects where
smoking impacts our health -- 50 or 60 damaging aspects, of which there are
many that can kill," says report author Dr. Sinead Jones, director of the
British Medical Association's Tobacco Control Resource Centre. "So the
evidence of fertility and conception -- for example, both male and female
fertility -- was important for us to highlight."
It finds women who smoke take longer to
conceive, and also will find their chances of conception reduced by up to 40
percent per cycle.
Also, both men and women may have less
response to fertility treatments when they smoke, thereby jeopardizing the
possibility of having a family.
"Men are twice as likely to be
infertile and to have damaged DNA in their sperm," Jones says. "And
with women, we found higher incidences of miscarriages."
The report says that between 3,000 and 5,000
miscarriages per year in the
It also found that 120,000 men in
According to the report, there is conclusive
evidence that women smokers face a variety of ailments: a higher risk of heart
disease when taking contraceptive pills; early menopause; and cervical cancer.
The danger is passed on to the child, too: placental complications; premature
membrane rupture; premature and low birth weight babies; and perinatal death.
Babies whose mothers smoked had a higher
risk of SIDS, middle-ear disease, respiratory illnesses, developing asthma in
those previously unaffected, and suffering asthma attacks in those already
affected.
The more tobacco the person consumed the
greater the adverse effect, the report notes, and stopping smoking dramatically
reduced the effects.
"This report clearly shows the
devastating impact of smoking on generations to come," says Deborah
Arnott, director of the British anti-smoking organization Action on Smoking and
Health. "Stopping smoking should be the number one priority for anyone who
wants to have children."
"This is important not just to increase
the chances of conception but also to give your child the best start in
life," she continues. "More than 17,000 children are hospitalized
every year [in the
But the report finds good news in the
growing trends towards eliminating tobacco advertising and promoting smoke-free
legislation in many areas, such as in the United States and in many European
cities.
"Our government has a long way to
go," Jones says. "We find that they are very complacent on the
issue."
Courtesy Andrew Conaway HealthDay Reporter
Black Youths Likelier to Quit Smoking
Study cites
parental disapproval, less exposure to peers who smoke
Most black teens
try smoking cigarettes, but they're much less likely than whites and Hispanics
to become regular smokers as adolescents and young adults, new research finds.
The Rand Corp.
study, published in the February issue of the American Journal of Public
Health, found 62 percent of black youths had lit up by age 13, compared with 69
percent of Hispanics, 52 percent of whites and 36 percent of Asian-Americans.
But by age 15,
just 7 percent of blacks in the study had become regular smokers, compared with
20 percent of whites and Hispanics and 8 percent of Asian-Americans.
"What we
find really intriguing is that this parental disapproval of smoking really
seems to have an impact that African-American kids really pay attention
to," says study author Phyllis L. Ellickson.
Ellickson,
director of the
For the study,
researchers tracked more than 6,000 blacks, whites, Hispanics and
Asian-Americans for 10 years, from ages 13 to 23.
Students
completed surveys about substance abuse, smoking and psychological, social and
behavioral factors.
By age 23, the
survey showed, 19 percent of blacks smoked regularly, compared with 32 percent
of whites, 29 percent of Hispanics and 16 percent of Asian-Americans.
Along with
influence of peers and parents, researchers looked at risk factors that could
be related to decisions on whether to smoke, such as school grades and
"problem behavior" such as rebelliousness and marijuana or alcohol
use.
Asian-Americans
did well in school and were less likely than others to drink alcohol, smoke
marijuana, or be exposed to "pro-smoking influences," Ellickson says.
Blacks, by
contrast, had significantly worse grades than whites throughout middle school
and high school. "But," Ellickson adds, "it appears to be
counteracted by positive influence from parents and less exposure to
smoking."
For example, the
proportion of black youths with a best friend who smokes dropped after age 13
or 14, the study says.
Edwin Fisher, a
professor of psychology, medicine and pediatrics at
"An
overlooked aspect of preventing smoking in adolescents is parental involvement
and parental wisdom in treating smoking as a health problem, not a discipline
problem," says Fisher, a spokesman for the American Lung Association.
"So it's not
a matter of simply saying, 'You don't smoke because you're my child and it's my
house.' It's a matter of explaining to young people why smoking is so
dangerous, and providing them opportunities for showing independence in doing
things their own way in healthy ways without needing to show their independence
by doing things like smoking."
Preventing
smoking during the teen years is critical. Tobacco use typically begins by age
16, and the first smoke almost always occurs before high school graduation, the
American Lung Association says. At least 4.5 million American adolescents
smoke, and each day 6,000
Adolescent
smoking has been linked not only to significant health problems, but also
involvement in fights, carrying weapons, engaging in high-risk sexual behavior
and using alcohol and other drugs.
Four decades
after the landmark Surgeon General's Report on Smoking and Health provided the
first official
The Dana-Farber
Cancer Institute, a teaching affiliate of
The findings
appear in the same issue of the American Journal of Public Health, along with
results of a separate Dana-Farber study on one of the first workplace programs
to successfully reduce smoking rates among blue-collar workers. The study
concluded that smoking cessation combined with broader occupational safety and
health worked much better than smoking cessation offered alone.
Researchers
tested the two approaches at 15
In an analysis of
national survey data from 1999 to 2001, the U.S. Centers for Disease Control
and Prevention found 8.2 percent of blacks aged 12 to 17 had smoked during the
preceding month. That compares with 29.5 percent of American Indians and
By
Genes May Help You Quit Smoking
Those with two
in particular have an easier time
Did you ever wonder why
some people stop smoking cold turkey and never look back, while others struggle
to quit again and again?
Researchers from the
Two genes in particular seem to help smokers
quit successfully, and this same combination of genes also makes them less
likely to start smoking again, report the researchers in the October issue of Health
Psychology.
"This study provides the first evidence
that genes that alter dopamine function may influence smoking cessation and
relapse during treatment," study author Caryn Lerman, associate director
for Cancer Control and Population Science at the
Dopamine is a neurotransmitter that acts as
a messenger between nerve cells in the brain.
Lerman and her colleagues studied 418 people
who were enrolled in a clinical trial to test the effectiveness of the
antidepressant bupropion for smoking cessation. The study participants either
received a placebo or bupropion for 10 weeks and behavioral counseling.
Blood samples were taken from all of the participants
for genetic analysis. Smoking status was assessed at the end of the 10 weeks
and then again after six months.
People who had particular variants of a
dopamine transporter gene (SLC6A3) and a dopamine receptor gene (DRD2) were
more successful at staying off cigarettes and avoiding relapse than people who
didn't have those variants.
"One of the great mysteries in smoking
cessation is why some people find it so easy and why it's so hard for
others," says Robert Baker, director of the Ochsner Center for the
Elimination of Smoking in New Orleans. "I hear about people who have
smoked for 40 years and then just put them down one day. Others haven't smoked
as long and seem to have a much harder time. I think genetic factors do play a
role."
Dr. Marc K. Siegel, an internist at
What's exciting about this research, Siegel
says, is the possibility that one day doctors could specifically target smoking
cessation treatment to each patient based on their genetic makeup. But such a
therapy is likely a long time away. "If you're waiting for a cure before
you quit smoking," advises Baker, "you may not live that long."
Despite some compelling reasons to quit --
including an increased risk of many cancers, heart disease and a one in five
chance of developing emphysema or chronic bronchitis, according to the American
Cancer Society -- many people still smoke.
About 25 percent of all men and 21 percent
of women in the
The good news is that plenty of people --
with and without these genes -- have quit smoking. The American Cancer Society
says that more than 44 million Americans have stopped smoking.
"You may have a more difficult time if
you don't have these genes," says Baker, "but you can still get off
cigarettes. I'm sure there are thousands upon thousands who have done just
that."
By Serena Gordon HealthDay Reporter
Decades After Landmark Smoking Report,
Some Issues Remain Clouded
Research
finds misuse of tobacco funds 40 years later
Forty
years to the day that a landmark Surgeon General's report found the health
hazards of smoking warranted "appropriate remedial action," a new
study says there is still a long way to go.
A
series of public health measures large and small have been taken since the 1964
report declared that cigarette smoking causes cancer and other diseases. Perhaps the single largest came in 1998, when the Master Settlement
Agreement (MSA) required four
The
original lawsuit, brought by state attorney generals, aimed to get funds for
Medicaid to recover the cost of treating tobacco-related illness. The
settlement, however, allowed the states to use the windfall primarily at their
own discretion.
And
while many states said that they planned to use the funds to defray Medicaid
costs, few have actually done so, according to new research being released
Sunday from the Jan. 15 issue of the New England Journal of Medicine.
The
journal chose this date because of
For
the most part, the researchers say, states have not used the funds to cover
Medicaid costs or for tobacco control and education projects. Instead, they
have been used to address budget deficits and ensure "no new taxes."
"We
missed a big opportunity, and we certainly could have done a lot more and we
didn't do it. That's a shame," says Dr. Steven A. Schroeder, author of the
new study and a professor of health and health care at the
"[The
tobacco industry] got out of it easy," adds Dr. Robert Giusti, chief of
pediatric pulmonology and assistant chair of pediatrics at
According
to the New England Journal article, in fiscal year 2003, 47 percent of the MSA
payments were funneled into state budgets, up from 29 percent the year before
and from 16 percent in the three preceding fiscal years.
Perhaps
most troubling, many states are mortgaging future MSA payments through bond
issues. This gives states a direct and strong interest in keeping the tobacco
companies afloat so they will continue to pay.
In
addition, certain stipulations in the original settlement, such as stronger
warnings on tobacco packages, have been abandoned.
Most
of the funding for the American Legacy Foundation disappears after five years
because the money depends on the tobacco companies' maintaining a 99.05 percent
or greater share of the
The
new findings coincide with the Jan. 6 release of the American Lung Association
State of Tobacco Control: 2003, which concludes that most states are not doing
what it takes to protect citizens from tobacco smoke. The report card gave an
"F" to 38 states and the
There
have been some forward movement, however.
The
article quotes Matt Myers, director of the Campaign for Tobacco-Free Kids,
saying that MSA was responsible for "the most significant increase in
spending on tobacco prevention and cessation in history. These funds have
forever changed the debate about the appropriate level of funding for tobacco
control."
The
MSA-funded American Legacy Foundation, Schroeder writes, is "the most
important national counter-marketing effort in 30 years."
And
to pay for all this, tobacco companies had to raise the price of cigarettes, an
action which in itself resulted in fewer smokers.
The
innovation from here on, Schroeder says, "is going to have to be on the
ground and a little bit at a time, and it's too bad."
Still,
there are hopeful signs. The telephone "quit lines," for instance, have
been "fantastic," Schroeder says. They just haven't been marketed
very well. Fuel for the anti-tobacco movement is also coming from raising
cigarette taxes, counter-marketing (such as the American Legacy Foundation),
and the clean indoor air movement.
Meanwhile,
Guisti, adds, getting people to quit smoking is still the primary
responsibility of physicians.
"I
think there are reasons for optimism," Schroeder says. "Smoking rates
are going down and smoking is becoming less socially acceptable. Those are two
wonderful trends, [but] the problem is a lot of people think the battle is over
-- but it's not."
His
argument is bolstered by another new body of research, released in Saturday's
British Medical Journal, that found low-tar cigarettes are no less damaging to
health than any other form of filtered cigarettes.
The
American Cancer Society estimates that before the 1964 Surgeon General's
report, about half of all American adults smoked; today, the organization says,
it's down to about 22 percent.
Smoking
kills 440,000 American men and women each year, which is almost one person a
minute, the ACS says. And cigarette smoking causes approximately 30 percent of
all cancer deaths in the country, it adds.
(Courtesy of Amanda Gardner,
HealthDay Reporter)
Smokers: Consider Your Legs
Blocked
arteries can lead to amputation
If
you're a smoker, you should worry about your legs, the Society of
Interventional Radiology warns.
What
with lung cancer, heart attack, stroke and the like, smokers have plenty to
worry about, the society acknowledges. But legs -- specifically, blood vessels
in legs -- often get ignored.
Just
as smoking accelerates the buildup of the fatty deposits in heart and brain
arteries that result in heart attacks and strokes, it has the same effect in
legs. The result is a condition called peripheral vascular disease (PVD), which
can lead to gangrene or amputation.
And
it's not only smokers who are at risk, says Dr. Ziv J. Haskal, a professor of
radiology and surgery at
"It
is an accepted belief that PVD is vastly under-diagnosed," Haskal says.
"It affects perhaps 10 million Americans. But it is often mistaken for
other conditions, such as arthritis."
The
classic symptom of PVD is intermittent claudication, leg pain that occurs when
walking or exercising and disappears when the activity stops. But many people
with PVD have other symptoms, such as numbness and tingling of the legs and
feet, ulcers or sores that don't heal, or coldness of the legs or feet.
Such
symptoms should send a person to a radiologist for a simple screening test
called an ankle brachial index, which compares blood pressure in the leg with
blood pressure in the arm, Haskal says. It is "an excellent diagnostic
test," he adds.
"Detecting
PVD doesn't mean that you can reverse it," Haskal says. "But its
progression can be stopped by a supervised exercise program and medication.
Such a program has been shown to improve walking distance."
For
severe cases, he says, an interventional radiologist can apply the same
techniques used for heart artery blockage -- angioplasty to widen the blood
vessel followed by implantation of a stent, a flexible tube, to prevent it from
closing.
And,
of course, a smoker should stop smoking if possible, Haskal says, because
"there are a thousand other reasons why someone should stop smoking."
(Courtesy of Ed Edelson, HealthDay
Reporter)
Heart Patients Gain by Quitting Smoking
Study
finds it's never too late to break habit
You have heart disease and chest
pain -- a heart attack waiting to happen. Quitting smoking is the least of your
worries, right?
Think
again. Heart disease patients who quit smoking can reduce their risk of
premature death by about 36 percent, regardless the severity of their illness
or their age, says a new study by British researchers.
"It
seems that it's always worth quitting," says study leader Julia Critchley,
an epidemiologist at the Liverpool School of Tropical Medicine in
Critchley
and a colleague, Simon Capewell of the
The
20 studies included more than 12,000 people, of whom nearly 5,700 were smokers.
Taken together, they showed that people who stopped smoking reduced their risk
of death by 36 percent compared with those who continued lighting up. The
so-called "relative risk" of suffering non-deadly heart attacks was
also lower, by 32 percent, in the groups that quit smoking. Follow-up periods
in the studies ranged from two years to 26 years. However, the risk of death
didn't fall with time, suggesting that most of the drop in risk associated with
quitting smoking occurs within two years or so of cessation.
A
report on the new study appears in the latest issue of the Cochrane Library, an
international medical publication.
Dr.
Richard Stein, a cardiologist at
Still,
Stein adds, the latest study sounds "reasonable" given what
researchers have found previously. The link, he says, is probably related to
the way tobacco smoke exacerbates trouble spots, or plaques, in narrowed blood
vessels. Smoking damages the cells that line vessel walls. When these cells are
the only thing keeping a "vulnerable" plaque from breaking loose into
the bloodstream, the added weakening can be devastating.
When
people stop smoking, they snuff out a major source of instability for their
vulnerable plaques -- and thus avoid future heart attacks and strokes, Stein
says.
If
you do quit smoking, ask for a raise.
Courtesy of Adam Marcus (HealthDay Reporter )
Smoking and Bladder Cancer in Women
A new study shows smoking puts women at significantly higher risk for
urinary bladder cancer.
Bladder cancer strikes nearly 55,000 people
in the
The study involved more than 27,000 women
who were participating in the Iowa Women's Health Study. All completed a study
questionnaire on various health-related factors in 1988 and then were followed
for the next 13 years to assess for bladder cancer incidence.
Results show current smokers had about a
5.5-fold higher risk of developing bladder cancer than nonsmokers. After
adjusting for other factors that could increase the risk, smokers still had
about a 4.25-increased risk. Quitting smoking helped. Women who had kicked the
habit for longer than 15 years had a relative risk approaching that of
nonsmokers.
The study also linked bladder cancer in women
to several other risk factors, including diabetes, lack of physical activity,
being unmarried, and having a smaller body mass index. However, these risks
were not as significant as the smoking risk.
SOURCE:
Cancer, 2002;95:2316-2323
Courtesy of Ivanhoe Newswire
Smokers Raise Risk of MS
Study
finds they're twice as likely to develop disease
Smokers
face twice the risk of developing multiple sclerosis (MS), a crippling disease
that destroys the lining of nerve cells, new research shows.
Norwegian
and American scientists have found people smoked -- including those who've quit
the habit -- have nearly double the risk of MS as those who never used tobacco.
The effect wasn't quite as great as the long-established impact of smoking on
the risk of cardiovascular trouble, such as heart attacks and chest pain, but
it was larger than the increased risk of asthma associated with tobacco use.
"We
found this rather strong relationship between smoking and MS. It's almost
comparable with cardiovascular disease" and smoking, says study leader
Trond Riise, an epidemiologist at the
Multiple
sclerosis involves the destruction of a protein called myelin that covers nerve
fibers -- probably by the body's own immune system. Myelin both protects nerves
and lets them function properly. People with MS suffer a wide range of symptoms
with varying severity. These include difficulty walking and swallowing, fatigue
and vision problems. The disease, which affects 400,000 Americans, usually sets
in between the 20s and 50s.
Scientists
aren't sure why smoking might heighten the risk of developing MS. One
explanation, Riise says, is that smoking saps the immune system and makes
people vulnerable to infections, particularly of the throat, that trigger the
nervous system disease. "We believe that it's most likely that the factor
that initiates this disease is an infection," Riise says, though he admits
that the mechanism remains "speculation." A report on the findings
appears in the Oct. 28 issue of Neurology.
A
2001 study by
Riise's
group looked at the risk of MS and smoking in 22,240 Norwegian men and women
living in
The
researchers identified 86 cases of MS. The risk of developing the disease was
80 percent greater among smokers or former smokers than among people who'd
never smoked.
The
association between smoking and the nerve disorder was greater for men than
women. It didn't appear to wane significantly in former smokers, although most
people had quit relatively recently before being diagnosed with MS, Riise says.
The average duration of smoking before diagnosis was about 15 years.
In
addition to raising the odds of developing MS and perhaps other autoimmune
diseases, previous research suggests smoking also appears to worsen flare-ups
of symptoms.
However,
Stephen Reingold, vice president of research programs at the National Multiple
Sclerosis Society, says the newest findings don't address that effect. "It
does not tell us anything about the impact of smoking for people who have
MS," he says.
Reingold
says smoking, infections and other environmental exposures or behaviors probably
interact with a genetic susceptibility to MS.
Courtesy of By Adam Marcus
(HealthDay Reporter)
Smokers: Beware Bad Air
Pollution
can triple heart attack risk, study finds
If
you're unwise enough to smoke, you'd better keep a close eye on local air
pollution levels, a French study indicates.
"We
clearly showed that the heart attack rate was increased by 161 percent when the
ambient air pollution index was high," says Dr. Yves Cottin, a professor
of cardiology at the University Hospital of Dijon, who presented the findings
Nov. 9 at the American Heart Association's annual conference in Orlando, Fla.
"Smokers are particularly sensitive to air pollution, since we found a threefold
increase risk in heart attack in the smoking population when the pollution is
high."
The
risk is closely associated with levels of fine particles, which mainly are
generated by diesel engines, the study finds.
Cottin
and his colleagues collected data on 322
The
pollution level rose to 6 or higher only 18 days of each year, but those days
had the greatest incidence of heart attacks, especially for smokers, Cottin
says.
Smokers
"should reduce or stop cigarette smoking during poor air quality
days," he says. "Smokers are also recommended to stay at home during
those days."
And
high pollution levels also call for special attention to the symptoms of a
heart attack on high-pollution days, in case immediate emergency care is
needed, Cottin says.
The
French report is the latest addition to "a host of short-term and
epidemiological studies that show an association between cardiovascular events
and air pollution," says Dr. Robert D. Brook, an assistant professor of
medicine at the University of Michigan and a member of an expert panel that is
writing a position paper on the subject for the American Heart Association.
"Certain
individuals are at especially high risk," Brook says. "They include
smokers, the elderly, people with diabetes and children, in relation to asthma.
This finding has been replicated all over the world, and an association has
also been found with the risk of stroke."
Cottin
says his group is studying the mechanism by which air pollution causes heart
attacks and other cardiovascular problems. There is evidence that pollutants
can contribute to an inflammatory process that leads to rupture of fatty
deposits called plaques, releasing clots that block blood vessels, he says.
Some
newspapers publish information on local air pollution levels on a regular
basis, Brook says. Air pollution readings for communities across the country
also are available daily on the Web site of the U.S. Environmental Protection
Agency.
Courtesty of Ed Edelson (HealthDay Reporter)
COPD: The Unnoticed Epidemic
Jump in cases fueled by women getting lung
disease
Most people have never heard of it, and have no idea what the acronym means.
But it's the fourth leading cause of death in the
COPD, short for chronic obstructive pulmonary disease, is essentially an umbrella term that refers to irreversible airflow obstructing and which includes chronic bronchitis and emphysema. Patients often say that they feel "hungry for air." The disease has no cure.
While death rates for other diseases include stroke and heart disease were decreasing, the mortality for COPD jumped 163 percent from 1968 to 1998. By 2020, experts say, it will be the third biggest killer in the world.
"It's a common disease that has reached epidemic proportions,"
says Dr. Richard S. Irwin, president of the
Women are driving that trend, adds Dr. A. Sonia Buist, a professor of
medicine at
About 24 million Americans are estimated to suffer from COPD, only 10 million of whom are diagnosed and only 6 million of whom are being treated. Those numbers help explain why November has been designated COPD Awareness Month, and why medical professionals are pushing for doctors and patients alike to recognize the disease in its own right.
Why the increase? Buist attributed it mostly to increases in smoking and in exposures to other risk factors, especially in developing countries, as well as to the changing age structure of the population. "More people are living into the COPD years," she says.
Smoking is, in fact, the number one cause of COPD, in the
Why are women increasingly affected? Because they started smoking and joining the workforce in the 1940s and are now seeing the result of those exposures.
The disease is grossly under diagnosed, even though diagnosis can be as
simple as spirometry, a classic breathing test that some argue should become
the fifth vital sign. "Only 15 percent of people with COPD in the
One of the problems is that we all lose lung function as we get older, and the symptoms of COPD too often are confused with those of normal aging. Those symptoms include shortness of breath, increased effort to breathe, chronic cough, increased mucus production and frequently clearing of the throat.
Once lung damage has happened, it can't be reversed. The best you can do is to stop the damage in its tracks, and the best way to do that is to (you guessed it) stop smoking. In fact, the only two things that have been shown to improve mortality are oxygen supplementation in people with low blood oxygen and quitting smoking.
Drugs such as bronchodilators and inhaled steroids can control various
symptoms but right now, that's it as far as pharmacotherapies go. "The
prospect of something novel soon is not particularly good," says Dr. Alan
R. Leff, a professor of medicine, pediatrics, anesthesia and critical care and
the
Exercise, however, does have benefits. It "doesn't change the lung but
it allows you to do more with the lungs you have," says Dr. Mark J. Rosen,
a professor of medicine at Albert Einstein College of Medicine in
Courtesy
of Amanda
Gardner HealthDay Reporter
Vitamin C May Ward Off Stroke
A study finds an added benefit for
smokers.
People who eat a diet rich in vitamin C may be at lower risk of suffering strokes, and smokers who do so may benefit the most.
A new Dutch study finds people with the lowest amount of vitamin C in their diets were 30 percent more likely to have a stroke than people with the highest amount of it.
People with the highest amount of vitamin C in their diets consumed more than 133 milligrams of vitamin C per day. People with the lowest amount in their diets got less than 95 milligrams per day. The recommended daily amount is 60 milligrams a day.
Smokers with diets high in vitamin C were more than 70 percent less likely to have a stroke than smokers with diets low in vitamin C.
Antioxidants such as vitamin C may protect cells from oxidative stress, which plays a role in stroke, the researchers say.
"The lower third will have a higher risk of stroke and those with
higher intake will be at lower risk," says study author Dr. Monique
Breteler of
The research "confirms that the healthy diet is good for you, one that is rich in antioxidants and vegetables, as we have seen over the last several years," she adds.
Researchers studied 5,197 people aged 55 and older living in
Participants were then tracked for an average of 6.4 years, and during that time, 253 of them suffered strokes.
The study also found smokers benefited from high levels of vitamin E in their diets. They were more than 20 percent less likely to have a stroke than those with diets low in vitamin E. Ironically, nonsmokers with high vitamin E levels didn't enjoy similar protection.
"This is not an excuse to continue smoking. There is more than enough medical evidence to show that smoking is extremely bad for you," Breteler cautions. "The effects of anti-oxidation are more than outweighed by other factors."
"But we looked at that because smoking causes damage due to increased oxidative stress. Then vitamin C has anti-oxidative properties, so we looked at [that] connection and saw that it was indeed the case," she says.
However, the use of dietary supplements containing vitamins C and E and other antioxidants didn't seem lower the risk of stroke more, but Breteler says this finding doesn't mean supplements have no potential benefit.
"I think it's important for the public to keep hearing the message
about our diet and reducing stroke risk, and this study shows this quite very
nicely," says Dr. Philip B. Gorelick, head of the cerebrovascular disease
and neurological critical care department at
The results appear in the Nov. 11 issue of Neurology.
This seems to confirm similar findings from a 2002 Finnish study, which showed a relationship between low vitamin C levels and an increased risk of stroke. The study of 2,419 men between the ages of 42 and 60 also showed a relationship between high levels of vitamin C and reduced stroke risk, especially in overweight and hypertensive men.
One possible explanation is that vitamin C enhances endothelial function, which inhibits artery clogging and lowers blood pressure. But the link could also simply be that people who take vitamin supplements or eat vitamin-rich fruits and vegetables may be more health-conscious than those who don't.
So the study cautions that vitamin C alone may not be responsible for the results of the study.
Rich sources of vitamin C include oranges and other citrus fruits, strawberries, red and green peppers, broccoli, and brussels sprouts. Good sources of vitamin E are vegetable oils such as sunflower seed, cottonseed, safflower, palm and wheat germ oils, margarine and nuts.
Vitamin C has had a much heralded history, ever since the 18th century British explorer James Cook was credited with being the first captain to use diet as a cure for scurvy, the disease caused by lack of ascorbic acids. After making his crew eat cress, sauerkraut and an orange extract, he lost no men to the ailment on several months-long voyages.
It has, it also seems, even reached a sort of cult status. One such example is the efforts of the former Nobel-prize winner Linus Pauling, who advocated, against medical evidence some say, megadoses of vitamin C to protect against cancer and many other ailments. Pauling died in 1994 at age 93.
But studies have shown that, since vitamin C passes out of the body via urine, amounts in excess of what the body can use are simply eliminated.
Courtesty of
What's in Cigarette Smoke?
Cigarette smoke contains over 4,000 chemicals, including 43 known cancer-causing (carcinogenic) compounds and 400 other toxins. These include nicotine, tar, and carbon monoxide, as well as formaldehyde, ammonia, hydrogen cyanide, arsenic, and DDT.
Nicotine is
highly addictive. Smoke containing nicotine is inhaled into the lungs, and the
nicotine reaches your brain in just six seconds.
Nicotine in small
doses acts as a stimulant to the brain. In large doses, it's a depressant,
inhibiting the flow of signals between nerve cells. In even larger doses, it's
a lethal poison, affecting the heart, blood vessels, and hormones. Nicotine in
the bloodstream acts to make the smoker feel calm.
As a cigarette is
smoked, the amount of tar inhaled into the lungs increases, and the last puff
contains more than twice as much tar as the first puff. Carbon monoxide makes
it harder for red blood cells to carry oxygen throughout the body. Tar is a
mixture of substances that together form a sticky mass in the lungs.
Most of the
chemicals inhaled in cigarette smoke stay in the lungs. The more you inhale,
the better it feels—and the greater the damage to your lungs.
Listed here are
109 of the more toxic chemicals. Those proven to cause cancer are in boldface
type.
|
|
*Courtesy
of QuitingSmokingSupport.com
Smoking Rate Dips
Among
The percentage of American adults
who regularly smoke cigarettes fell slightly in 2001, according to a federal
study. The numbers cast doubt on the nation's ability to meet a targeted
reduction of the habit by 2010.
About 440,000 Americans die
each year from lung cancer and other diseases related to tobacco use, making
smoking the leading preventable cause of death in the
In 2001, an estimated 46.2
million adults, or 22.8 percent of those 18 years and over, reported that they were
current smokers, according to an annual survey published on Thursday by the
Centers for Disease Control and Prevention.
That compared to an
estimated 23.3 percent of adults who smoked the previous year and 25 percent
who did in 1993. Blacks in particular registered sharp declines in smoking in
2001, according to the survey.
CDC officials welcomed the
findings, attributing them in part to the impact of anti-tobacco control
programs at the state level, but they also warned that not enough money was being
invested in such efforts.
Tobacco companies agreed in
1997 and 1998 to pay $206 billion as part of a landmark legal settlement with a
number of states that had sued the industry to recoup the health-care costs of
treating sick smokers.
"The states were
starting to fund some comprehensive tobacco-prevention and control programs,
but unfortunately with the budget crises those funds are being lost and put
into general revenues," said Dr. Corinne Husten, medical officer in the
CDC's office of smoking and health.
UNLIKELY TO MEET TARGET
"We do have a lot of
concern that we may not be able to maintain these (smoking) declines,"
said Husten, who added that the United States was unlikely to meet a federal
goal of reducing the adult smoking rate to 12 percent or less by 2010.
To hit that target, adult
smoking would have to fall more than four times the rate of decline between
1994 and 2001.
The CDC is advocating that
states increase the funding and implementation of comprehensive anti-tobacco
programs that target different ethnic communities, adolescents and rich and
poor Americans alike.
Anti-tobacco activists
contend that the human and economic costs of smoking could be dramatically
reduced if authorities at both the state and federal levels clamped down on
tobacco advertising and raised taxes on cigarettes to make them less
affordable, particularly to teenagers and young people.
In the past two years about
half the state governments in the nation have increased excise taxes on
cigarettes and other tobacco products. A number of others have passed
legislation further restricting smoking in restaurants and public areas.
Earlier this year, an
advisory committee to the U.S. Department of Health and Human Services
recommended increasing the federal cigarette tax by $2 a pack and using at
least half the revenue to help people kick the habit.
The Bush administration
rejected the idea.
"We urge the White
House to reconsider its position in light of the clear need for bold and aggressive
efforts at all levels," Matthew Myers, president of the Campaign for
Tobacco-Free Kids, a Washington-based anti-tobacco group, said on Thursday.
SOURCE:
Morbidity and Mortality Weekly Report
Magnetic Field May
Help Smokers to Quit
Smokers exposed to repeated
pulses of magnetic energy via a coil-shaped stimulator placed on the head
apparently smoke less afterwards, German doctors report. This technique, called high-frequency
repetitive transcranial magnetic stimulation (TMS) may eventually be used to
reduce cigarette smoking among individuals who want to quit.
Repetitive TMS, sometimes
used to treat depression, "is a novel approach that has never been tried
before" for smoking cessation, lead author Dr. Peter Eichhammer told Reuters
Health. Drugs, such as bupropion or
nicotine replacement, are commonly prescribed for patients when they decide to
stop smoking. Eichhammer explained that his team studied TMS because it
specifically "targets areas related to the brain's reward system."
Hence, TMS avoids side effects caused by drugs that affect other areas of the
brain not involved in cravings.
The research team at the
University of Regensburg, Germany, conducted a trial in a group of 14 smokers
who wished to stop smoking. According to their report in the Journal of
Clinical Psychiatry, each subject underwent two trials of active stimulation
and two trials of "sham" stimulation on 4 consecutive days, without
knowing which was which.
On average, the subjects
smoked significantly fewer cigarettes during the 6-hour period immediately
following active treatment compared with placebo treatment. No adverse effects
other than two cases of mild headache after active stimulation were reported.
The German research team
has initiated a larger trial of repetitive TMS as treatment for smoking
cessation. In addition, Eichhammer said, "We want to optimize
high-frequency repetitive TMS as an effective method for treating other
addictions as alternatives to conventional drug-related treatment approaches."
SOURCE: Journal of Clinical
Psychiatry, August 2003.
Smoking and Litter
A frequently overlooked
aspect of smoking is the ever-growing problem of litter. The following is an excerpt from www.cigarettelitter.org a non-profit
organization dedicated to reducing cigarette-related litter. Please check out their site and you might
find out some new information about the multiple dangers of the use of tobacco
products!
There
is a lot of misinformation out there regarding cigarette butt litter. The
biggest myth is that cigarette filters are biodegradable. In fact, cigarette
butts are not biodegradable in the sense that most people think of the
word. The acetate (plastic) filters can take many years to decompose. Smokers
may not realize that their actions have such a lasting, negative impact on the
environment.
This myth has been perpetuated not
just by the wishful thinking of many smokers, but also by the cigarette
companies, who have taken great pains to keep their customers in the dark on
this issue. It is very common for highly littered items such as soda cans,
snack wrappers, and fast food containers to have a simple "Please Don't
Litter" message. You won't find such a message on cigarette packs. Although
our contacts in the industry are at a loss as to why they can't take this
simple step, our best guess is that they would prefer to leave their customers
blissfully ignorant. Maybe they think that people will smoke fewer cigarettes
if they have to be responsible for disposing of them. We think they ought to
give their customers the benefit of the doubt. Smoking and littering do not
have to be synonymous, as many smokers have proven by example.
What happens after that butt gets casually flicked
onto the street, nature trail, or beach? Typically wind and rain carry the
cigarette into the water supply, where the toxic chemicals the cigarette filter
was designed to trap leak out into aquatic ecosystems, threatening the quality
of the water and many aquatic lifeforms. Cigarette butts may seem small, but
with several trillion butts littered every year, the toxic chemicals add up!
Study Affirms Safety of The Pill
But news isn't so good for
smokers who took the early versions of oral contraceptive
There's good news for women
who were early users of birth control pills in the 1970s and 1980s as well as
for women now taking newer versions of oral contraceptives.
A large, decades-long study
confirms that nonsmoking women on the pill do not have higher overall death
rates. Although mortality rates from cervical cancer were higher, these were
balanced out by decreased death rates from ovarian and other uterine cancers.
Smokers have a much more
grim prognosis, however. The study, appearing in the July 19 issue of The
Lancet, found that overall death rates were more than twice as high for women
who took the pill and who smoked at least 15 cigarettes a day as compared to
nonsmokers.
Two other large studies had
already published similar results. "This is a pretty solid finding with
these big studies in agreement," says Dr. Martin Vessey, lead author of
the latest study. "The sound statistical conclusion is that there is no
harmful effect to taking oral contraceptives. That's a very important result."
Vessey, an emeritus professor of public health at the
The study started by
recruiting 17,032 British women between 1968 and 1974. At the time, the women
were aged 25 to 39 and were white and married. All used oral contraceptives, a
contraceptive diaphragm, or an intrauterine device (IUD). Many of the women
ended up being on the pill for at least eight years, Vessey says.
"In common with a
number of studies, we did find an increase in deaths from cancer of the cervix
in pill users," Vessey says. "That was compensated for by fewer
deaths from cancers of the other parts of the uterus and from cancers of the
ovary. If you put those three reproductive cancers together, the net effects of
the pill on the three is beneficial."
"Their findings are
consistent with previous studies, and that is a slight increase in cervical
cancer and a decrease in particular in ovarian cancer. We've pretty much known
this for many years now," adds Dr. Sanjay Agarwal, director of the Center
for Reproductive Medicine at
Heavy smokers, however, had
more than double the death risk, largely from heart disease and stroke.
"The key to this study
is the breakdown effect of smoking. It really does underline the significant
detrimental effects of smoking even in young ages," Agarwal. "This
study just highlights very strongly that smoking really does increase the risk
of heart attacks and hemorrhagic stroke in women taking birth control
pills."
So what does it mean to
today's pill users? "This study mainly concerns the pills used in the '70s
and '80s, and in
For middle-age and early
elderly women who were on the pill during this time period, the results should
be very reassuring -- as long as they're not smokers.
"I think you could
definitely regard these findings as also being reassuring in terms of modern
pills, although obviously there is a bit of extrapolation there," Vessey
says.
"We would assume that
lower doses equate with more safety, so I think this is encouraging,"
Agarwal adds. "I think the main areas where oral contraceptives are likely
to be safer are with stroke and heart attacks."
Another study is looking at
this very thing. And, meanwhile, the current researchers will continue to
collect data from this study.
Courtesy of Amanda Gardner
SOURCES: Martin Vessey, M.D., emeritus
professor of public health, University of Oxford, Oxford, U.K.; Sanjay Agarwal,
M.D., acting director, division of reproductive endocrinology, and director,
Center for Reproductive Medicine, Cedars-Sinai Medical Center, Los Angeles;
July 19, 2003, The Lancet.
Smoke Screen
Study: Tobacco use in movies spurs teens to smoke
Smoking on the silver screen strongly encourages
adolescents to start puffing themselves, new research says.
The study finds that adolescents exposed to more
smoke-filled films are far more likely to take up smoking over the next two
years than their peers who don't watch such movies.
"Smoking in the movies is associated with about
125,000 children a year dying prematurely," says Stanton Glantz, director
of the Center for Tobacco Control Research and Education at the
Making smoking on screen a trigger for an
"R" rating would cut that 125,000 figure in half, says Glantz, author
of an editorial accompanying the journal article. "The question is, does
the Motion Picture Association of America [MPAA] want to save 63,000 lives a
year with appropriate ratings?" he says.
Many previous studies have suggested that depictions
of smoking on screen encourage teens to smoke. Indeed, the World Health
Organization declared "tobacco-free films" a theme of this year's
World No Tobacco Day.
Harder to prove, however, is a direct connection
between a teen seeing smoking in a movie and his or her decision to pick up the
habit. The latest study sought to determine how often that happened.
A research team led by Madeline Dalton, a professor of
pediatrics at
"We picked them based on box office receipts, not
on whether they had smoking,"
Over the next 13 to 26 months, 259 (about 10 percent) of
the boys and girls reported smoking at least once. But while 17 percent of
those in the group that saw the most movies with smoking tried tobacco, only 3
percent in the group that saw the fewest such films did so.
Risk-seeking behavior, rebelliousness, self-esteem,
parental history of smoking, and other personality and parenting factors
affected the chances that a child would start smoking. After weighing these
factors, the researchers determined that seeing smoky movies still nearly
tripled the odds a youth would experiment with tobacco -- a greater effect even
than cigarette advertising, Glantz says.
"We found that of the children who tried smoking,
half of them did so based on what they saw in the movies,"
Since smoking is rarely integral to movie plots,
Glantz says, people should wonder why characters are often lighting up.
"Sex and violence sell tickets. Smoking doesn't. Why are [movie studios]
clinging to it?"
The MPAA did not return calls seeking comment.
Tobacco industry documents reveal that cigarette
makers in the past have forged deals with
Kimberly Thompson, a Harvard epidemiologist who has
studied tobacco use and movies, calls the new study "important"
because it's the first thorough attempt to put a time-frame around youth
smoking and exposure to the habit on film. However, she says, the researchers
fall short of sealing their case.
"A strong correlation still doesn't get you to
causation. This is good and strong evidence, but it's still a
correlation," Thompson says.
By Adam Marcus
HealthDay Reporter
Studies Rap Philip Morris on Gay Marketing
In two new
reports, researchers claim the Philip Morris tobacco company tried to extend its
advertising reach into the gay community in the early 1990s while denying it
was targeting any specific group.
"They were trying to have it both ways. They want the market, they want the business, but they want to buy our silence and distance themselves when homophobes object to their involvement," says Naphtali Offen, co-author of one of the studies and a research associate at the LGBT (Lesbian, Gay, Bisexual & Transgender) Tobacco Project at the University of California at San Francisco (UCSF).
Philip Morris also turned a boycott led by
gays into a public relations opportunity by boosting its funding for AIDS
organizations, the researchers say.
But a spokesman for Philip Morris defends
the company, saying it markets its product -- which he acknowledges is
"addictive" and "causes serious disease" -- to all kinds of
groups and has advertised for years in gay-oriented magazines. In regard to the
boycott issue, spokesman Brendan McCormick says the company has a history of
supporting charitable organizations, including those that fight AIDS.
Today, tobacco companies actively pitch
their products to gays through advertising in magazines and newspapers, and the
market seems to be receptive. Studies have shown gays and lesbians are more
likely to be smokers than heterosexuals.
But tobacco companies weren't always
interested in advertising directly to gays. In 1992, Philip Morris became the
first tobacco company to buy ads in a gay-oriented magazine.
But the groundbreaking ads in a magazine
called Genre, geared toward gay men, created a stir. Philip Morris
responded to media requests by saying it didn't target "specific groups in
society," researchers report in the June issue of the American Journal
of Public Health.
That, the researchers charge, was
disingenuous. An examination of internal tobacco company documents found that a
marketing consultant in early 1992 urged the company to advertise its Benson
& Hedges cigarette brand in gay publications.
The documents were released in 1998 as part
of a settlement between the attorneys general of several states and the tobacco
industry.
The consultant wrote that the company could
target the gay community and that "you can own this market." The
company agreed to do so, "but when they got called on it, they said they
really didn't even see [Genre] as a gay magazine," says study
co-author Elizabeth A. Smith, a research associate at UCSF's LGBT Tobacco
Project.
Philip Morris continued to advertise in gay
publications throughout the 1990s. "Our marketing efforts are designed to
appeal to diverse people of both genders and all ethnic groups and sexual
preferences," McCormick says.
In another report, in the June issue of Tobacco
Control, researchers at the
The boycott was launched by the
The boycott, against Marlboro cigarettes,
had no major effect on the earnings of Philip Morris, the researchers say. But
the company did respond by boosting its funding of AIDS organizations and the
chapter ended its boycott efforts, even though Philip Morris still supported
Helms.
"The boycott that was initially against
the industry ended up being an opportunity for [Philip Morris] to make friends
by settling the boycott," Smith says.
McCormick, however, says Philip Morris has
long supported charities, including those involved in health efforts. In fact,
he says, the tobacco company even supports efforts to educate people about the
risks of smoking.
"We manufacture a product that causes
serious disease in smokers and is addictive," he says. "The safest
thing for people to do is not for smoke at all."
However, he adds, 45 million Americans
haven't made that choice.
Meanwhile, the company went a step further Tuesday
toward accepting more government regulation. Mike Szymanczyk, chief executive
of Philip Morris, told a Congressional panel that oversight from the U.S. Food
and Drug Administration (FDA) would let the company sell two products that are
less harmful than cigarettes, according to an Associated Press report.
The company had long opposed any government
regulation over tobacco, but changed course in 2000, saying it would be
amenable to some oversight. However, the U.S. Supreme Court ruled that year
that the FDA had no authority.
SOURCES: Naphtali Offen and Elizabeth A. Smith, Ph.D., research associates, LGBT Tobacco Project, University of California at San Francisco; Brendan McCormick, spokesman, Philip Morris, New York City; June 2003 American Journal of Public Health; June 2003 Tobacco Control
Courtesy: By Randy Dotinga HealthDayNews
Reporter
Smoking Increases Panic Attack Risk
Studies in the past suggested an
association between smoking and mental disorders. Now, new research finds a
unique connection between smoking and the risk of a panic attack.
For the research, authors used data from
the Early Developmental Stages of Psychopathology Study. The study included
adolescents and young adults in
At the start of the study researchers
note a clear association between panic attacks and disorders and regular
smoking and nicotine dependence. After analyzing the data, researchers say they
also found an increased risk for the onset of a panic attack in those who
smoked regularly and were nicotine dependent. Prior nicotine dependence also
increased a person's risk for the onset of a panic disorder, whereas those who
had panic problems did not show a tendency to turn to smoking.
Researchers say this study shows a rather
unique and specific relationship between smoking and the increased risk for a panic
attack or panic disorder. They say their results suggest smoking and nicotine
dependence increase the risk for panic attacks and disorder but not for most
other anxiety disorders. Furthermore, prior smoking increases the risk for a
panic problem, but there is no higher incidence of smoking among cases with an
anxiety disorder.
SOURCE:
Archives of General Psychiatry, 2003;60:692-700
Smoking on the Big Screen
Now researchers in New Hampshire say
parental guidance can impact what movies kids see, and, in turn, their exposure
to harmful habits. It's clear the presence of smoking by celebrities in movies
influences adolescent attitudes and behavior.
Movies traditionally glamorize smoking,
associating it with character traits such as toughness, rebelliousness, and
sexiness, the research explains. Past research has shown adolescents are
responsive to actions, including smoking and drinking, portrayed on screen. The
influence of the media in this situation, finds research, can be very powerful.
James D. Sargent, M.D., and his team of researchers at
Nearly 5,000 junior high school students
participated in the study. The students reported which of the 50 randomly
chosen movies they had seen. The researchers then analyzed the occurrence of
smoking in these films. In general, the students who had the most exposure to
smoking in movies had the least amount of parental restriction and the greatest
access to movies, including movie channels available at home. Dr. Sargent
concludes, "Exposure to movie smoking is reduced when parents limit movie
access" and monitor the films they allow their child to view.
Dr. Sargent proposes that a new approach to the exposure of movie smoking "may be to limit access of young adolescents to movies," because adolescents who saw fewer smoking depictions also saw fewer movies in general.
SOURCE: Archives of Pediatric & Adolescent Medicine
2003;157:643-648
Banning Smoking in the Home Helps Infants
Banning smoking in the home limits
infants' exposure to tobacco smoke. Infant exposure to environmental tobacco
smoke increases the risk of sudden infant death syndrome, asthma, and other
respiratory conditions.
A recent study analyzed the urinary
cotinine levels, a byproduct of nicotine, of 314 infants living in smoking
households. Participating infants were between 4 weeks and 24 weeks old.
Researchers from the University of Warwick, United Kingdom, found banning
smoking in the home was associated with a small but significant reduction in
cotinine levels. Other methods to reduce tobacco smoke in the home, such as no
smoking while the infant sleeps or limiting the number of cigarettes, produced
no reduction in the cotinine levels and had no effect on exposure of infants.
More than 80 percent of participating
parents thought environmental tobacco smoke was harmful and 90 percent believed
that their children could be protected from smoke exposure in the home. At
least half of the parents reported using more than one measure to reduce infant
tobacco smoke exposure in the home. Further research is needed to determine if
measures less strict than banning smoking, like opening windows and using fans
while smoking will have any effect on infant cotinine levels.
SOURCE:
British Medical Journal, 2003;327:257-260
Courtesy
of (Ivanhoe Newswire)
Smoking and Oral Contraceptives: A
Deadly Combination
A new study shows oral
contraceptives are safe for non-smokers but can be deadly for women who smoke.
The study began 35 years ago and included 17,000 women.
Oral contraceptives were widely used in the
1970s and 1980s. There has long been a question of whether being on the birth
control pill could increase your chance for cancer or other fatal diseases. As
part of the Oxford Family Planning Association study, researchers from the
The women in the study were between 25 and
39 years old. They either used oral contraceptives, a contraceptive diaphragm
or an intrauterine device. Follow-up information was available on the women up
until 2000. By that time, researchers report 889 of the 17,000 women had died.
Researchers looked at the cause of death and which contraceptive they used.
The study reports there was no increased
risk of death among the women who used the birth control pill compared to the women
who never used oral contraceptives. In fact, the numbers suggest the death rate
was lower among those who were on birth control pills. However, there was an
increased risk of death from heart disease in women who used the oral
contraceptive and smoked. Specifically, there was a 25-percent increased risk
of death for light smokers. The study also found women who smoked more than 15
cigarettes a day and were taking oral contraceptives were twice as likely to
die than non-smokers.
Researchers say this study confirms what
three other studies have found in that there is no adverse effect from oral
contraceptive use in non-smokers. Study authors say this should be a reassuring
finding for many older women today. However, the study also confirms that
smoking and oral contraceptive use can be a deadly combination.
This article was reported by Ivanhoe.com,
who offers Medical Alerts by e-mail every day of the week. To subscribe, go to:
http://www.ivanhoe.com/newsalert/.
SOURCE: The Lancet, 2003;362:185-191
Teaching Blue-Collar Workers to Kick Butts
Blue-collar
workers have traditionally had the hardest time trying to kick the smoking
habit. But researchers have found a new method that doubles the success rate
for those who want to quit.
The study, published in the August issue of the journal Cancer Causes and Control, found that blue-collar workers are more willing to quit when they're taught about the risks of combining smoking with other common workplace hazards.
"We're trying to catch their
attention," says the study's lead author, Glorian Sorensen, a
"Blue-collar workers have a harder time
quitting. And more traditional workplace programs haven't been as successful
with blue-collar workers," she says.
There's a pressing need for a successful
cessation program because blue-collar workers smoke far more than other
workers. A 1997 study found that 37 percent of male blue-collar workers and 33
percent of female workers smoked. For white-collar workers, just 21 percent of
men and 20 percent of women smoked, Sorensen says. Moreover, white-collar
workers are quitting at a faster rate, she says.
But the risks of smoking on the job aren't
just limited to cigarettes for blue-collar workers. Those workers are often
exposed to chemicals that can become deadlier when combined with smoking. For
example, asbestos workers who smoke dramatically increase their chances of
dying of lung cancer, the American Lung Association says.
Even without smoking, American workplaces
can be dangerous. An estimated 60,000 people die of occupational diseases every
year; of those, more than 17,000 die of lung cancer because of inhaling
cancer-causing agents, the American Lung Association says.
Those factors increase the urgency of
persuading blue-collar workers to quit, Sorensen says.
In prior studies, she found that blue-collar
workers get less support in their efforts to quit than white-collar workers,
even though they're often very willing to try.
"Blue-collar workers attempt to quit at
the same rate as white-collar workers, but they're much less successful. Maybe
there is more peer pressure in these workplaces," adds Greg DeLaurier, a
consultant with the
For the Dana-Farber study, researchers
randomly selected 15 large manufacturing companies around the
Twice as many workers in the latter group
quit smoking over the 16-month study, Sorensen found. And because they were
already careful about workplace hazards, they were much more willing to support
their co-workers' efforts to quit smoking.
DeLaurier has had the same experience in
working with blue-collar smokers.
"What doesn't work very well is if you
just offer a generic smoking program," he says. "But if you tie it
into the specifics of the workplace, smoking is no longer just an abstraction.
It puts it in a context the worker will listen to."
The study also supports the idea that the
work environment is an ideal place to tackle health issues, Sorensen says.
"The large majority of adults spend
their time in a work setting. It's a place that shapes our behavior through
social norms and the support you get from your co-workers," she says.
"As we think about health, whether smoking or anything else, we need to
think about how those individual factors are situated in the broad fabric of a
person's life."
What To Do
To learn more about occupational hazards and
their long-term effects, visit the American
Lung Association. For information about smoking on the job, visit this site. To
read one of the first federal reports about the risks of smoking in blue-collar
work sites, try the Centers
for Disease Control and Prevention.
SOURCES:
Glorian Sorensen, Ph.D., professor of health and social behavior, department of
health and social behavior, Harvard School of Public Health, and director,
Dana-Farber Institute's Center for Community-Based Research, Boston; Greg
DeLaurier, labor consultant with the University of Massachusetts, Lowell;
August 2002 Cancer Causes and Control. By Ross
Grant HealthScoutNews Reporter
Smoking Cessation and Its Benefits
Description
Quitting smoking can have a profound, positive impact on a person's quality of
life.
Data from large prospective studies have
shown that cigarette-smoking men have a 70 percent higher overall death rate
than nonsmokers. The excess mortality of female smokers has been somewhat less
than that of male smokers, but is increasing.
A strong dose-response relationship exists
between cigarette smoking and excess mortality, as measured by the age at onset
of smoking, the number of cigarettes smoked, the number of years smoking, and the
depth of inhalation. Cessation of smoking is associated with a decrease in
excess mortality.
Treatment
Speak with your physician about quitting smoking. He or she will help you
through the process, answer your questions, and give you support.
Nicotine replacement therapy is available
(nicotine patch, nicotine gun, and nicotine nasal spray) after you have quit.
Other medications may be helpful as well.
Questions To
Ask Your Doctor
Are there tests that will show the status of my lungs?
Will there be weight
gain if smoking is stopped?
Are there any
medications to help a person stop smoking?
What are their side effects?
Is nicotine
addicting?
Will there be
increased nervousness when a person stops smoking?
Does genetics
have anything to do with smoking?
Does smoking
cause permanent staining of the teeth?
What are the pros and cons of the nicotine patch, nicotine gum, and nicotine nasal spray?
Passive Smoke Tied to Dental Woes in Kids
Study finds
link, but expert sees no association
Parents have yet another reason to quit smoking: Passive smoke from
their puffing could be ruining their children's baby teeth.
That's what researchers from the University of Rochester Medical Center in
In the March 12 issue of the Journal of
the American Medical Association, the
"This is just one more piece of
evidence that passive smoke harms children," says study author Dr. C.
Andrew Aligne, who was with the University of
Rochester Medical Center at the start of the study but finished it after
founding a company called Pediathink.
Aligne says further research needs to be
done to corroborate their findings, but adds, "if this relationship is
causal, one quarter of children with cavities in their baby teeth would be
cavity-free if tobacco smoke exposure could be eliminated."
However, Dr. Manuel Cordero, a
Despite advances in dental care, tooth decay
remains a common childhood disease, costing the
The researchers gathered data on 3,531
children between the ages of 4 and 11 for this study from the Third National
Health and Nutrition Examination Survey. All of the children had a complete
dental examination and blood tests that measured their cotinine levels.
Cotinine is a byproduct of nicotine that is present in the blood of people who
are exposed to smoke, either directly or indirectly.
Fifty-three percent of the children had
cotinine levels high enough to indicate passive smoke exposure, according to
the study. Nearly half of all the children had at least one decayed or already
filled baby tooth, while 26 percent already had a cavity in one of their
permanent teeth.
Children exposed to passive smoke had almost
twice the risk of having a cavity in their baby teeth, according to Aligne.
However, there was no statistically significant relationship between cavities
in permanent teeth and passive smoke. While the researchers weren't able to
address the reason why with the data available, Aligne believes that as with
other health risks, younger children and their developing bodies are simply
more susceptible.
Cordero points out the researchers found
that cavities in baby teeth were nearly three times as common in kids whose
parents had less than a high school education compared to those with more than
a high school education. This factor, he says, is probably more of an influence
on cavity development than passive smoking.
Aligne, however, says he and his colleagues
tried to control the data for other potential risk factors -- such as poverty,
race, sugar intake and family income -- and that they still found an
association between passive smoke and cavities in baby teeth after doing so.
In the study, the researchers explain it may
not necessarily be the smoke exposure, but that parents who smoke may also have
other unhealthy behaviors, such as not brushing teeth regularly or eating too
much candy, which could be causing the cavities.
Cordero believes these explanations are much
more likely. "Parents who smoke are teaching poor overall health
habits," he says.
Whether the connection between passive smoke and cavities holds up in future studies or not, Aligne says, "Dental cavities and passive smoking are still very big public health problems and we need to do more to prevent them."
Source: By
Serena Gordon, HealthScoutNews Reporter
Temporary Symptoms May Cause Some to Relapse
Smokers are likely to develop mouth ulcers and cold symptoms for up to two weeks after quitting. This problem, which researchers say is temporary, may be one reason so many succumb to nicotine's urges.
But if smokers trying to quit can hang on, all symptoms seem to be gone after six weeks, according to new research. The study is published in the February issue of Tobacco Control.
Researchers followed the progress of 174 smokers wanting to quit. The smokers went through a seven-week smoking cessation program combining behavior support with nicotine patches.
After weeks one and two, there were significant increases in mouth ulcers and cold symptoms, such as coughing, sneezing, and sore throats. It was during this time, according to researchers, that people were more likely to have setbacks. Slightly less than half the participants managed to resist temptation for the entire six weeks of the study.
The researchers say that mouth ulcers may be caused by the loss of antibacterial properties of smoking while an increase in cold symptoms may be due to a loss of natural antibodies in the saliva.
Michael Ussher, MD, and colleagues, conclude that more research is needed to determine if cold symptoms and mouth ulcers persist beyond two weeks after quitting.
Being psychologically prepared for these effects may improve smokers' odds of quitting, they say.
SOURCE: Fern Garber - WebMD News Tobacco Control, February 2003.
Can Lung Cancer Be Prevented?
Retinoid May Help Prevent Lung Cancer - Vitamin A
Derivative May Lower Risk Among Former Smokers
by Jennifer Warner (WebMD Medical News )
Quitting smoking is the single biggest thing a person
can do to reduce their risk of lung cancer, but now researchers may have
finally found a way to lower the risk for people who have already quit their
cigarette habit. A new study shows that daily treatment with a retinoid drug
may prevent lung cancer in former smokers.
Retinoids are natural and synthetic compounds related
to vitamin A (retinol) and retinoic acid (RA). Although they have been found to
help prevent head and neck cancers, until now retinoids have not been shown to
be effective in preventing lung cancer.
In fact, researchers say some studies have shown that
retinoids are of no benefit in reducing the risk of lung cancer in current
smokers. But this may be the first study that has shown a benefit in targeting
former smokers and reversing signs of precancerous lesions in lung tissue.
Lung cancer is the leading cause of cancer death in
the U.S., and researchers say about 90% of all lung cancers occur in people who
smoke, which has made smoking cessation efforts a major focus of lung cancer
prevention efforts.
Although the risk of lung cancer decreases in people
who quit smoking, the risk still remains about twice as high as those who have
never smoked, for about 20 years after they quit. The risk after 20 years
lowers some but continues to remain high.
In the study, published in the Feb. 5 issue of the
Journal of the National Cancer Institute, researchers looked at the effects of
two different types of retinoids on restoring the presence of a substance
called retinoic acid receptor beta (RAR-beta) in lung tissue from a group of
226 former smokers. Loss of RAR-beta is considered a sign of pre-cancerous
tumors.
Researcher Jonathan M. Kurie, MD, of the University
of Texas M.D. Anderson Cancer Center in Houston, and colleagues found a loss of
RAR-beta in nearly 60% of the participants at the start of the study.
But after three months of twice-daily treatment with
the retinoid known as 9-cisRA, there was a significant increase in the presence
of RAR-beta among those who received the retinoid compared with the placebo. No
benefit was found for the second type of retinoid tested.
Researchers say the study shows that the benefits of
retinoid treatment may differ among current vs. former smokers.
In an editorial that accompanies the study, Jason S.
Vourlekis, MD, and Eva Szabo, MD, of the National Cancer Institute, say it
remains to be seen how restoration of RAR-beta might correlate to a reduction
in risk of lung cancer, and more studies will be needed to examine that issue.
SOURCE: Journal of the National Cancer Institute,
Smokers have more aches and pains!
As if lung cancer, heart disease, and emphysema
weren't enough, researchers now say smoking may be to blame for some common
aches and pains, too. A new study shows smokers are more likely to complain
about pain in their back, neck, arms, and legs than non-smokers.
The report, published in the January issue of the
Annals of Rheumatic Diseases, shows smokers as well as ex-smokers are at higher
risk for aches and pains -- especially those that lead to chronic disabilities
and interfere with daily activities.
Researchers surveyed nearly 13,000 adults across
They found the percentage of people who reported
pain in the past year was consistently higher among smokers and ex-smokers for
all the parts of the body examined by the study.
Smokers and ex-smokers were at especially high
risk for pain that prevented them from performing daily tasks.
Researcher K. T. Palmer, MD, of the
But researchers say the pattern persisted even
when they adjusted for these factors and when they looked at pain reported
among only white-collar workers.
Even so, they say it's unclear whether tobacco
affects the body's pain sensors, or whether people with a low tolerance for
reporting pain and disability are more likely to take up and keep smoking.
"If taking up smoking increases pain
susceptibility, then this provides another reason to avoid the habit,"
according to the researchers, "but if the type of people who smoke report
pain more readily, a search should next be made for the underlying
mechanisms...."
~Jennifer Warner
Nicotine Replacement Backed Despite Cancer Study
Researchers say they're still much safer than smoking
By Randy Dotinga
Nicotine replacement products are much safer than
smoking despite a new study suggesting that nicotine could play a role in lung
cancer.
That assurance comes from a leading maker of these products as well as researchers who reported last week that nicotine appears to give a helping hand to cancer cells in the lungs.
"Our study is probably the first to show that nicotine can act similarly to a carcinogen," says Kip A. West, a researcher with the National Cancer Institute.
However, the study is based on findings in the laboratory, and researchers haven't tested their theories on animals or humans. And the scientists aren't suggesting that smokers give up trying to quit with the aid of nicotine replacement products, which now include lozenges in addition to the ubiquitous patches and gum.
To make the point even clearer, GlaxoSmithKline issued a statement saying the risks of using nicotine-based smoking cessation products "are extremely small compared to the known deadly risks of smoking." The pharmaceutical company makes NicoDerm CQ nicotine patches, Nicorette gum and Commit lozenges, which let smokers slowly wean themselves off their addiction by getting doses of nicotine without having to light up.
According to the American Cancer Society, the nicotine replacement products deliver lower doses of the chemical than tobacco. They also let smokers focus more on the psychological difficulties of quitting than the physical addiction.
While nicotine is considered to be largely responsible for turning smokers into addicts, scientists have not considered it to be a cause of cancer. Instead, researchers blame hundreds of other poisonous chemicals in cigarettes, pipes and cigars.
Federal researchers, however, wondered whether nicotine could play a role in the development of cancer. They set up experiments involving lung cells in a laboratory and report their findings in a recent issue of the Journal of Clinical Investigation.
In a healthy body, cancer-infected cells will automatically activate a kind of suicide program: The cells will kill themselves before they can wreak havoc on the body. However, when researchers hit human lung cells with cancer-causing chemicals, the levels of nicotine normally experienced by smokers appeared to prevent the cells from switching on the suicide protocol.
"It has a protective effect," West says. The survival of the cells, in turn, "allows them to accumulate mutations that would enable them to become tumor cells."
The researchers found that nicotine and a related chemical in tobacco known as NNK appear to affect the cells by influencing pathways where command signals travel.
What does this mean for nicotine products that are geared to help people stop smoking? West says the research does raise concerns if people use the products for a long time. "Prolonged use could be a bad thing," he says.
GlaxoSmithKline says its products are designed to be used over 10 to 12 weeks as a "step-down therapy" that more than doubles the chances of successfully quitting over the "cold turkey" approach.
However, the company suggested that long-term use might not be a problem. It cited a 1997 federally funded study that found people could safely take nicotine gum for five years.
What To Do
For a fact sheet on nicotine replacement products, go to the American Lung Association or the American Cancer Society.
SOURCES: Kip A. West, Ph.D., postdoctoral fellow and researcher, Cancer Therapeutics Branch, National Cancer Institute, Bethesda, Md.; statement from GlaxoSmithKline; Jan. 1, 2003, Journal of Clinical Investigation
Copyright © 2003 ScoutNews, LLC. All rights reserved.
Study: 'Safer' Cigarettes May Be All Smoke
Two studies find targeted brands may lead to
increased addiction
By Jennifer Thomas
HealthScoutNews Reporter
They're sold by big tobacco companies and go by
names like Advance, Eclipse and Accord.
They're marketed as safer cigarettes that can lessen the risks of smoking by releasing fewer cancer-causing substances.
But two new studies show these so-called safer cigarettes may not be safer at all -- and may even lead to increased addiction.
In the first study, researchers invited 20 smokers in the lab and, over three days, had them puff on their own brand of cigarettes, then an Advance cigarette, now sold by Brown & Williamson Tobacco Corp., and also an unlit cigarette for comparison.
Advance cigarettes are marketed as a safer cigarette because they supposedly
contain less of a type of cancer-causing substance called nitrosamines, said
Thomas Eissenberg, an associate professor of psychology at
The Advance study, which did not look at nitrosamine levels, found the cigarette produced 11 percent less carbon monoxide. Carbon monoxide has been linked to cardiovascular disease in smokers, Eissenberg said.
But Advance also delivered 25 percent more nicotine into the blood than the smokers' own brands. Nicotine is the addictive substance in cigarettes.
"We don't know for sure if it causes increased dependence, but certainly many smokers would like to know if they're being exposed to more nicotine," Eissenberg said.
A spokesman for Brown & Williamson responded that the researchers had looked at an early version of Advance cigarette made by a different company.
"The nicotine levels they are reporting are not correct," spokesman Marc Smith said. "They are looking at a product that is not on the market today. The product being sold today has much lower nicotine levels ..." He did not say what the nicotine levels were.
The study appears in the December issue of the journal Tobacco Control.
In a second study, published in the December issue of Harm Reduction, Eissenberg and his colleagues conducted a similar experiment with Accord cigarettes, made by Philip Morris Co. Inc., and Eclipse, made by R.J. Reynolds Tobacco Co..
Both cigarettes heat rather than burn tobacco, presumably reducing carcinogen levels.
Researchers didn't look at carcinogen levels, but they did look at nicotine, carbon monoxide and the effects on smokers' heart rate.
On the plus side, they found Accord delivered significantly less nicotine and boosted smokers' heart rate and carbon monoxide levels less than traditional cigarettes.
But Accord didn't do as well as traditional cigarettes in suppressing cravings or reducing such withdrawal symptoms as anxiety, restlessness and irritability, they found.
If Accord fails to give smokers the same satisfaction they get from smoking their regular brand, they may simply smoke more, which would defeat the purpose of safer cigarettes, Eissenberg said.
Eclipse, on the other hand, increased heart rate and suppressed withdrawal symptoms about as well as conventional cigarettes. However, Eclipse delivered about 30 percent more carbon monoxide than regular cigarettes, Eissenberg said.
"Based on our evaluation, all three alternative cigarettes appear to reduce some toxins that are associated with smoking-related diseases," Eissenberg said. "But our testing also revealed that Eclipse and Advance may increase levels of dangerous substances produced by these cigarettes that smokers should be aware of."
A spokeswoman for R.J. Reynolds said the 30 percent increase in carbon monoxide (CO) cited in the study is not correct.
"The CO claim mentioned in the study is contrary to what we have found during our extensive investigations. Under FTC machine-smoking puffing conditions, the 'tar' and nicotine yields for Eclipse are in the range of ultra-low-'tar' cigarettes, while the CO yield is in the low-'tar' range," said Carole Crosslin.
The company's extensive studies, she added, "have found that, on average, there is about a 10 percent increase in COhB in smokers switching to Eclipse from their usual brand."
However, Patrick Reynolds, founder of the Foundation for a Smokefree America, called the research an important step in debunking claims of safe cigarettes.
"There is an array of tobacco products on the market all claiming to varying degrees to be safer," said Reynolds, the grandson of R.J. Reynolds and the son of a man who died of smoking-related disease. "It will be decades before we have the medical data and studies in about whether these products are substantially safer."
Even if a product delivers less carbon monoxide or carcinogens, he added, it is still unknown what amount causes an individual smoker to get cancer or heart disease.
"Whether the products are one percent safer or 15 percent safer, we really don't have any clue," Reynolds said. "The big danger is that many smokers may believes these products are far safer than they really are and will justify their continued smoking based on that."
Hiking Cigarette Tax Could Save Millions Of Lives
Raising price seen as most effective way to cut
smoking-related deaths
By Jennifer Thomas
HealthScoutNews Reporter
What's the single most effective way of
preventing deaths from smoking?
Hike the price of cigarettes, new research says.
Raising the tax on cigarettes could avert between 5 million and 16 million tobacco-related deaths worldwide in the coming years, according to a study in the September issue of Nicotine & Tobacco Research.
Researchers evaluated the effectiveness of several types of tobacco control: tax increases; nicotine replacement; and a package of interventions, including bans on advertising and promotion of tobacco products, anti-smoking education and smoking restrictions in public places or work places.
They then used economic models and the results of previous smoking cessation studies to estimate the number of deaths that could be avoided by using the three methods around the world. These results were applied to a global model of smokers in 1995.
Raising the price of cigarettes by 10 percent worldwide would prevent between 5 million and 16 million deaths, they found. People in low- to mid-income countries and people between the ages of 15 and 29 would be the most impacted by the price increases, according to the study.
"In general, price increases are the most cost-effective, anti-smoking
intervention," writes lead author Dr. M. Kent Ranson, of the London School
of Hygiene and Tropical Medicine in
John Banzhaf, executive director Action on Smoking and Health, says the study is consistent with previous research.
"There are many studies which show that increasing taxes on cigarettes is a very effective way to decrease consumption," Banzhaf says. "And it's no surprise that they are most effective with kids and with people who are in the lower socioeconomic classes."
Nicotine replacement includes products such as chewing gum, skin patches, nasal sprays, inhalers and lozenges. Liberalizing access to nicotine replacement could avoid 1 million to 5 million smoking-related deaths, the study found. It would have the greatest impact on people between 30 to 59 years old.
Bans on advertising, prohibition of smoking in public places and anti-smoking educational programs would probaably reduce smoking worldwide by about 2 percent, meaning another 5 million lives would be saved.
In the
Peter Jacobson, an associate professor of health law at the
However, Jacobson adds, the study underestimates the power and importance of education programs that "de-normalize" smoking, making it a habit that is socially unacceptable.
This change in attitude toward smoking is largely a result of ceaseless efforts by educators and public health experts to spread the message about the dangers of tobacco, says Jacobson, lead author of Combating Teen Smoking: Research and Policy Strategies.
"One might get the false impression from this study that the only thing that's needed is to raise taxes," Jacobson says. "What's missing, and what many tobacco control researchers are starting to look at, are more comprehensive programs."
Raising taxes is but one, albeit important, weapon in the arsenal against tobacco.
He points out that smoking rates are higher in
European countries than in the
What about smokers' rights?
Banzhaf puts little stock in their arguments that they're being overtaxed. He cites a CDC study that found each pack of cigarettes will mean subsequent health-care costs of about $12.85. Much of that cost is paid for by non-smokers in the form of taxes and higher health-care costs, Banzhaf says.
In the state of
"It's a small step in the right direction to make them pay their fair share of these huge costs," he says.
What To Do
For more information on the legal battle against tobacco, upcoming anti-smoking legislation and the latest tobacco research, visit Action on Smoking and Health.
The Centers for Disease Control and Prevention has tips on quitting smoking.
SOURCES: John Banzhaf, executive director, Action on Smoking and Health, Washington, D.C.; Peter Jacobson, J.D., M.P.H., associate professor, health law, University of Michigan, Ann Arbor; September 2002 Nicotine & Tobacco Research
Copyright © 2002 ScoutNews, LLC. All rights
reserved.
All it
takes is one cigarette !
Up to now, it was thought it took a few years for smokers to become addicted, but the latest research shows addiction takes place in days
Experts have tried for
years to determine how long people have to smoke before becoming addicted, said
Dr Richard Hurt, director of the Nicotine Dependency Unit at the Mayo Clinic in
the
"The best answer to date has been one to two years," said Dr Hurt, who was not involved with the latest research. "There's been a suspicion that many people become addicted very quickly, but this is really the first hard evidence that we've had that this occurs."
Research reported in
the British Medical Association journal, Tobacco Control, found that several
12- and 13-year-olds showed evidence of addiction within a few days of their
first cigarette.
Dr Hurt said the findings would help scientists better understand the biology of nicotine addiction and lend more plausibility to the idea that some people may be more susceptible genetically to it than others.
The study was
conducted by scientists at the
The researchers did not label any of them as addicted because the standard definition of nicotine dependence assumes that addiction cannot happen without prolonged heavy smoking.
The scientists simply recorded symptoms that indicate addiction. Symptoms include cravings, needing to smoke more to get the same buzz, withdrawal symptoms when not smoking, feeling addicted to tobacco and loss of control over the number of cigarettes smoked or the duration of smoking.
A total of 95 teens said they had started smoking occasionally - at least one cigarette a month - during the study.
The scientists found that 63 per cent of them had one or more symptoms of addiction.
A quarter of those with symptoms got them within two weeks of starting to smoke and several said their symptoms began within a few days.
Sixty-two per cent said they had their first symptom before they began smoking every day, or that the symptoms had made them start smoking daily.
"The really important implication of this study is that we have to warn kids that you can't just fool around with cigarettes or experiment with them for a few weeks and then give them up," said Dr Joseph DiFranza, who led the research team.
"If you fool around with cigarettes for a few weeks, you may be addicted for life." - AP.
*courtesy of QuitSmoking.Com
Turns Out Secondhand Smoke, Not Curiosity, Can Kill a Cat
Study underscores the
threat to humans, especially children
WEDNESDAY, July 31
(HealthScoutNews) -- Even having nine lives is no protection against secondhand
smoke.
Cats who
live with people who smoke are more than twice as likely as other cats to
develop a deadly form of cancer called feline lymphoma, says a study by
scientists at Tufts University School of Veterinary Medicine and the
The study appears in
tomorrow's issue of the American Journal of Epidemiology.
The finding provides
compelling evidence of the need for further study of the link between
secondhand smoke and non-Hodgkin's lymphoma in humans, which is similar to
lymphoma in cats, the study authors say.
"We believe the
feline exposure patterns to environmental tobacco smoke may mimic those of
young children living in households where adults smoke and where the children
inhale tobacco smoke or ingest particulate matter by mouthing contaminated
objects," says lead author Elizabeth R. Bertone, an epidemiologist at the
University of Massachusetts at Amherst.
The study looked at 180
cats treated at
The authors adjusted for
age and other factors and concluded that cats exposed to any household
environmental tobacco smoke had 2.4 times greater risk of lymphoma than cats
who lived with non-smokers.
The risk increased with
longer exposure. Cats subjected to at least five years of secondhand smoke were
3.2 times more at risk for lymphoma than other cats.
The number of smokers in
a house also made a difference. One smoker in a home increased a cat's risk by
1.9 times, while two or more smokers made a cat 4.1 times more likely to
develop lymphoma.
Cats living in homes
where people smoked a pack or more of cigarettes a day were 3.3 times more at
risk than cats in smoke-free homes.
New Link Between Smoking
& Cancer Found
By Richard Woodman
LONDON (Reuters) - British researchers said on Tuesday they had identified a
possible new mechanism that might explain how smoking can cause breast and
bowel cancer as well as lung cancer. The team, at the
"We are excited about the findings of this research as they indicate a
possible new mechanism to explain the development of some cancers," said
research leader Dr. Andrew Renehan.
"This has potential implications for cancer risk assessment and cancer
prevention strategies in the future," he added in a statement.
The findings were presented at the British Endocrine Societies' meeting in
The team looked at cigarette smoking histories in over 400 individuals, aged 55
to 65, attending a bowel cancer screening trial in
"The findings were dose-related and were statistically significant,"
he added in a telephone interview. "There was a 20% to 25% difference in
IGF levels between the heaviest smokers and the non-smokers."
Asked about the likely biological mechanism, he said it was known that growth
factors could encourage cancer cell growth and protect abnormal cells against
natural death caused by apoptosis, the "cell suicide" mechanism.
However, he said that a much larger study would be needed to prove that
smoking, IGF levels and cancer risk are all linked.
Three studies released last year by British and American researchers suggest
that common processes involving insulin signaling control the ageing process in
organisms ranging from yeast to quite possibly humans.
Nicotine Patches, Gums May Pose Health
Risk : Nicotine By-Product Could Cause Problems
By Jennifer Warner
Nicotine patches and gums have helped millions of people improve their health
by allowing them to quit smoking. But a new study shows that these products may
create other problems for their users.
The study, published in the Journal of the American Chemical Society, shows
that nornicotine, a product created by the breakdown of nicotine, may interfere
with a variety of chemical reactions in the body. These reactions may, in turn,
trigger a range of negative health affects.
Researchers stress that their findings are preliminary and have only been
demonstrated in the lab, not in humans. The study suggests that those who take
medications or smoke while using nicotine products may be at a greater risk for
adverse drug reactions because nornicotine may alter the effects and potency of
other drugs.
While the addictive effects of nicotine is well known, the authors say their
study shows another by-product of tobacco also plays a role. Nornicotine can
prompt reactions that change the ways chemicals are processed and circulate in
the body, although nicotine has no effect on these reactions.
In fact, researchers say it's the first time this type of compound has been
shown to trigger these chemical reactions.
Some medications, such as steroids and antibiotics, may be more likely to
interact with nornicotine, according to researchers. Tests are now underway to
determine exactly which drugs may put smokers and users of other nicotine
products at risk.
Experts say love of nicotine is all in
mind
By Ronald Kotulak, Tribune science reporter
Working to unravel a long-standing puzzle of
cigarette addiction,
Published Thursday in the scientific journal Neuron, the research shows that
nicotine not only stimulates pleasure in the brain's reward center but has the
unique ability to neutralize the "off-switch" that usually throttles
down good feelings quickly.
The finding provides major clues to understanding the complex process by which
the brain becomes addicted to nicotine and opens new approaches to developing
drugs to block nicotine's power to hijack the brain.
For the 2,000 teenagers a day who become smokers, the new evidence helps to
explain how a single cigarette quickly teaches the brain cells of a first-time
smoker to crave nicotine.
And for the more than 30 million American smokers who try to quit smoking each year
and fail, the finding shows why breaking the habit is so hard.
The
It does so first by quickly turning on the pleasure chemical dopamine in the
brain's reward center, something scientists have known for several years. But the dopamine surge ends quickly, and researchers couldn't
figure out what caused nicotine's long-lasting high and its ability to induce
addiction.
McGehee's finding shows for the first time that nicotine also acts on a group
of regulatory cells whose job is to stop the dopamine high. With this control
mechanism temporarily disabled, the reward system continues to operate long
after it should have been shut down.
The result is a runaway feel-good sensation that the brain commits to its
memory bank as something it wants more of.
"This gives an explanation for why the long high happens," said Dr.
Glen Hanson, acting director of the National Institute on Drug Abuse.
"It's a combination of tolerance happening to several systems at the same
time. When you sum everything up, you get an enhancement of the dopamine
pleasure pathway."
McGehee's detailed studies of rat brains revealed the step-by-step process by
which nicotine takes over the brain's reward system. Neuronal pathways in that
system were examined cell by cell to determine how they responded or failed to
respond to individual neurotransmitters.
Drug companies have been hampered in their efforts to develop anti-addiction
medicines because they didn't know how the brain became addicted, said John
Dani, a Baylor College of Medicine neuroscientist who was one of the first to
show nicotine's effect on dopamine.
"Dan's work will allow both academic and pharmaceutical researchers to
focus on the mechanisms of addiction with a greater understanding of how they
work," Dani said.
The brain's reward system, scientists believe, is basically designed to help a
person learn what is good for his survival and what is not.
It provides a wide range of sensations from euphoria to just plain feeling
good. Experiences such as falling in love, getting a big promotion, coloring between the lines for the first time, seeing your
baby's smile and winning the lottery promote some of the biggest dopamine
jolts. Eating a good meal, making a new friend, taking a walk on the first
morning of spring, working a crossword puzzle and other less intense learning
experiences get less of the pleasure chemical.
"These really important events in our lives have a different quality to
them that is imparted by the reward system," McGehee said. "What the
drugs of abuse are doing is usurping that reward system."
Dopamine is carefully dispensed. A jolt makes a person feel good and helps lay
down a memory of a new experience or reinforce an old one.
But dopamine is soon cut off, reducing the pleasurable effect to baseline
levels. If it weren't turned down, dopamine would cause a constant feeling of
being high, which would impede new learning and reduce the chance of survival.
"Nicotine acts as if it's reinforcing a behavior that should be
rewarded," Dani said. "The brain is fooled into thinking that
nicotine is a proper participant in life."
An estimated 57 million Americans smoke, which is linked to more than 400,000
deaths annually from cancer, heart attacks, strokes and emphysema. It is the
nation's most preventable cause of death.
A cigarette contains about 10 milligrams of nicotine. About 1 to 2 milligrams
get into the blood stream and hit the brain's reward center within 10 seconds
after inhalation.
An average smoker takes 10 puffs per cigarette over a five-minute period. For a
person who smokes 1 1/2 packs daily, his brain gets 300 hits of nicotine.
That nicotine plugs into receptor ports on brain cells stimulating the
production of dopamine. Dopamine then turns the brain's pleasure center on.
At the same time, nicotine molecules plug into another set of inhibitory
neurons, jamming their ability to turn off the pleasure center. The subsequent
high lasts about an hour, the time it takes for nicotine in the blood to
subside to the point where the inhibitory system can be reactivated.
"There's no other outcome than excitation when you've got nicotine in the
system," he added. "It would be hard to design a drug that acts on
the reward center that would be more effective than nicotine."
Copyright © 2002, Chicago Tribune
Smokers Disillusioned With Their Habit
If They Could Start Over, Most Say
They Would Never Start By Jennifer Warner
WebMD Medical News
March 8, 2002 -- Given the chance, most smokers say they would have never
started smoking in the first place, according to a new survey of British
smokers. Many may also overestimate their plans to quit.
When asked: "If you had your time again, would you start smoking?"
83% of current smokers said they would not. Older adults seemed the most
disenchanted with their habit, with 90% of smokers aged 45 to 64 saying they
would not smoke if they could start over.
Researchers say that sense of regret may come with age because many of the
smoking-related health problems such as emphysema begin to surface later in
life.
The national survey of 893 smokers also revealed that most smokers aren't
realistic when it comes to thinking about quitting. Nearly 60% said they
planned to quit within two years, but recent history shows only about 6%
actually manage to do so.
Young smokers were especially optimistic about quitting. Eighty percent of
smokers under the age of 40 said they believed they would stop smoking within
20 years. On average, they thought they would quit within 2 years.
But those hopes may not be realistic, judging from previous research. In 1998,
65% of people that had ever been a smoker were still smoking at age 40 and 45%
at age 60.
The survey is published in this week's British Medical Journal.
How common is it?
--------------------------------------------------------------------------------
- SMOKING has been identified as the single most preventable cause
of death and disease in the
- Approximately 50 million Americans smoke
- There are over 1.1 billion smokers worldwide!
- They consume about 540 billion cigarettes each year
- 1.1 trillion cigarettes are smoked every year worldwide!
- Approximately 400,000 people die each year in the
- About 3 million people die worldwide each year, with about one-third of them in developing countries.
- Tobacco use rings up $50 billion each year in health care costs in
the
- Cigarettes currently cause approximately 20% of all deaths in
By Age
- In General the earlier someone starts smoking, the less likely that he/she will quit
- Smoking among high schoolers is increasing with more whites than blacks picking up the habit among juveniles
- 23.4% of people between 18 and 24 years of age smoke
- 25.9% of people between 25 and 44 years of age- the highest over all
- 23.4% of people 65 years or older smoke
For Teenagers
- Out of all the people who smoke, 80% started before the age of 21. This means that, you are more likely to start smoking as a teeenager than at any other age.
- Smoking in the teenage population starts usually around grade 6 and almost about 75% of teenagers who smoke now started around grade 9, according to a study done in 1986.
- Those teenagers who started smoking are at a much higher risk for drug abuse including cocaine and marijuana, than those who didn't start smoking.
By Sex
For Men
- THE #1 CAUSE OF DEATH IN MEN TODAY IN THE
- If you are over 35 and smoke, you are 10 TIMES MORE likely to get Chronic Obstructive Pulmonary Disease (COPD) and 22 TIMES MORE likely to die from Lung Cancer than those who do not smoke.
- Smoking is on the rise in young men, unfortunately.
- Men (23.9%) smoke more than women (21%)
For Women
- Deaths due to Lung Cancer have become higher than Breast Cancer since 1987.
- If you are 35 or over and smoke, you are 10.5 TIME MORE likely to get Emphysema or Chronic Bronchitis than nonsmoking females
- Those females who are starting to smoke are doing so at an earlier age than before.
- Babies are more likely to have birth complications if born to a woman who smoked during pregnancy than those who didn't.
- The number of women who smoke is increasing in many countries.
By Race
Blacks over 18 years of age have the highest amount of smokers
- Whites 22.9%
- Blacks 25.1%
- Hispanic 21.2%
- Asian 14.4%
By Education
- People with less formal education tend to smoke more
- Less than 12 years 29.1%
- More than 12 years 18%
By Location
- States with the highest cigarette taxes, such as
- States with the lowest cigarette taxes, such as
- In developed countries, 41% of men and 21% of women regularly smoke cigarettes.
- In developing countries, 50% of men smoke, and 8% of women.
SOURCE: The Ashtray: Smoking and Tobacco Abuse
Fighting Smoke With Smoke
No-Nicotine Cigarettes -- Quitting
Tool or Trap for Fools?
By Daniel DeNoon
Coming soon to a store near you: nicotine-free cigarettes. Smoking them is
supposed to help you quit smoking.
This isn't the first time that the tobacco industry has come up with this idea.
The soon-to-be-renamed Philip Morris Co. Inc. couldn't sell cigarettes made
from tobacco treated to remove nicotine. Vector Tobacco Inc. recently began
selling the "reduced carcinogen" Omni cigarettes. Now Vector has a
new almost-no-nicotine product made from genetically engineered tobacco plants.
It's slated for release some time this year.
Why would anybody smoke this high-tar, no-nicotine product -- even if, as
advertised, they taste like full-nicotine cigarettes? The idea is that these
"no-nics" might satisfy the urge to smoke while at the same time
weaning a person from nicotine. Can it work?
That depends on whom you ask. So far, the only researcher to look at how the
new tobacco product might help people quit smoking is Jed E. Rose, PhD, a
neuroscientist at
"I think it is a very seriously promising approach that needs to be
explored," Rose tells WebMD. "A lot of people jump to conclusions
based on the presumed motives of the tobacco companies. Whether it works is a
scientific issue, not a political one. There is widespread acceptance of the
theory that people smoke because they are dependent on nicotine. So if you
remove nicotine, it might possibly be a step toward quitting. It needs to be
tested and it may or may not work."
Other observers are far less impressed with the idea. One of them is Jeff
Wigand, PhD, the former cigarette company executive who blew the whistle on his
former employers.
"The way to help smokers to quit is to help them get over their nicotine
addiction -- and this is best done with help from people who have the person's
heath as their first interest, not a tobacco company," Wigand tells WebMD.
"When has a single tobacco company got into the smoking-cessation
business? Now we are going to give out cigarettes as a quitting strategy? If
smokers need something to hold in their hands, give them a pencil."
Randolph D. Smoak Jr., MD, immediate past president of the American Medical
Association, says nicotine-free and reduced-carcinogen cigarettes are just
marketing gimmicks.
"A cigarette is nothing but a delivery device for premature death,"
Smoak says. "No matter how you dress it up or dress it down, it is the
same product. If you take away the nicotine, then people are not going to smoke
it, because they do not get the nicotine kick. If people are still smoking
cigarettes without nicotine -- if they will -- they still are exposed to the
carcinogens. To say we will take away the addictive portion is no salvation. To
diminish the nicotine is just a false sense of security and hope for people who
are addicted and are exposed to carcinogens."
In a study being presented to the
Smokers who use low-tar, low-nicotine cigarettes puff harder to get a
satisfactory smoke. But Rose found that these same smokers take normal puffs of
high-tar, no-nicotine cigarettes. And the no-nics satisfied smokers' craving
for cigarettes -- although it didn't keep them from getting the bad mood that's
part of nicotine withdrawal.
Rose says that cigarettes give a smoker a quick nicotine "spike."
This acts as a reward and makes a smoker want another cigarette. Rose says that
no-nic cigarettes don't have that reward -- so smoking them might eventually
break the vicious smoking-reward circle.
"Whether those internal cues to keep smoking extinguish over time, that is
the big unknown," Rose says. "If it turns out to be a period of weeks, that would be great. If it took
years [of smoking no-nic cigarettes], it would not be so great. We just
don't know the answer to that question yet."
Rose's study was partially funded by an unrestricted gift to
'Light' Cigarettes - Not Better
Smoking "light" cigarettes may
seem like a healthier alternative to regular cigarettes, but according to a
recent
The Facts in General
- About 400,000 Americans die every year because of health problems due to smoking
- 1 out of every 6 deaths each year are due to smoking.
- Every year, 1.5 million people quit smoking but 50 MILLION KEEP ON GOING!!
- Tobacco companies spend $5,000 every minute to advertise their products
- Smoking has caused the health care costs to rise dramatically to $65 billion per year.
- Smoking CAUSES Emphysema, Lung Cancer, and Chronic Bronchitis
Warning Labels
Fifty-eight percent of smokers interviewed in the study said full-color
pictures of how cancer affects the mouth, lungs, heart
and brain had made them think more about the health effects of smoking.
The warnings were so effective that 44 percent of the smokers polled said the
new warnings increased their motivation to quit smoking. And 38 percent of
smokers who attempted to quit in 2001 said the new warnings were a factor in
motivating them to try to quit.
The full-color, picture-based warnings cover half of the front and back of each
package of cigarettes. They include pictures of a diseased mouth, a lung tumor,
a brain after a stroke, a damaged heart, and a limp cigarette that warns of
impotence. Warnings inside each package offer tips on quitting.
The warnings were launched about a year ago and replaced black-and-white text
messages that covered about 35 percent of each package, similar to cigarette
package warnings in the
The study also found that:
-- 43 percent of smokers and 40 percent of nonsmokers said they are more
concerned about the health effects of smoking because of the new warnings;
-- 21 percent of smokers said they have been tempted on one or more occasions
to have a cigarette but decided not to because of the new warnings;
-- 27 percent of smokers said they smoke less inside their home because of the
new warnings;
-- 35 percent of smokers and 34 percent of nonsmokers said they know more about
the health effects of smoking than they did before the new warnings;
-- 48 percent of nonsmokers said the new warnings made them feel better about
being a nonsmoker;
--17 percent of smokers said they have put their cigarette pack away at least
once because they did not want others to see the warning, and 24 percent of
smokers said they have at least once put a cardboard sleeve over their pack or
transferred cigarettes to another container;
--18 percent of smokers said they have on at least one occasion asked for a
different package of cigarettes when purchasing them because they did not like
the warning on the package first offered.
In addition, smokers and nonsmokers identified the warning depicting a diseased
mouth and the picture of a lung tumor as most effective at discouraging
smoking.
The health warnings on cigarette packages are required under the Tobacco
Products Information Regulations. The rules, which set a precedent at the time,
were adopted under the Tobacco Act that the Canadian Parliament passed in 1997.
In January 2000, similar bills were proposed in the
However, Reps. James V. Hansen, R-Utah, and Marty Meehan D-Massachusetts said
Wednesday that they will introduce legislation to require larger, picture-based
health warnings on
According to the Canadian Cancer Society,
The study, in which 2,000 Canadian adults were interviewed -- 633 of them
smokers -- was funded by the
Is smokeless tobacco safer than cigarettes?
It's true that many people think smokeless tobacco (also known as chewing or spit tobacco, or snuff) isn't as bad as cigarettes. One study quoted in the Surgeon General's Report (SGR) said that 77 percent of kids thought cigarette smoking was very harmful, but only 40 percent thought smokeless tobacco was very harmful. Very wrong! The truth is that smokeless tobacco use is connected with all sorts of problems.
BAD HEALTH!
Smokeless tobacco can cause bleeding gums and sores of the mouth that never heal. Eventually you might end up with cancer.
TOUGH TO QUIT!
Tobacco is tobacco: it all contains nicotine, and nicotine is addictive!
VERY DISGUSTING!
It stains your teeth a yellowish-brown color. It gives you bad breath. It can make you dizzy, give you the hiccups, even make you throw up. (Definitely NOT cool!)
Finally, one more fact to chew on -- according to the SGR, kids who use
smokeless tobacco are more likely to start using cigarettes, too. That's a
double whammy that no healthy body can survive! So spit it out; say no to
smokeless tobacco.
Cigarettes and the Digestive System
Cigarette smoking causes a variety of life-threatening diseases, including lung
cancer, emphysema, and heart disease. An estimated 400,000 deaths each year are
caused directly by cigarette smoking. Smoking is responsible for changes in all
parts of the body, including the digestive system.
This fact can have serious consequences because it is the digestive system that
converts foods into the nutrients the body needs to live.
Current estimates indicate that about one-third of all adults smoke. And, while adult men seem to be smoking less, women and teenagers of both sexes seem to be smoking more. How does smoking affect the digestive system of all these people?
Harmful Effects
Smoking has been shown to have harmful effects on all parts of the digestive system, contributing to such common disorders as heartburn and peptic ulcers. It also increases the risk of Crohn's disease and possibly gallstones. Smoking seems to affect the liver, too, by changing the way it handles drugs and alcohol. In fact, there seems to be enough evidence to stop smoking solely on the basis of digestive distress.
Heartburn
Heartburn is common among Americans. More than 60 million Americans have
heartburn at least once a month, and about 15 million have it daily.
Heartburn happens when acidic juices from the stomach splash into the
esophagus. Normally, a muscular valve at the lower end of the esophagus, the
lower esophageal sphincter (LES), keeps the acid solution in the stomach and
out of the esophagus. Smoking decreases the strength of the esophageal valve,
thereby allowing stomach juice to reflux, or flow backward into the esophagus.
Smoking also seems to promote the movement of bile salts from the intestine to
the stomach, which makes the stomach juice more harmful. Finally, smoking may
directly injure the esophagus, making it less able to resist further damage
from refluxed material.
Peptic
Ulcer A peptic ulcer is an open sore in the lining of the stomach or
duodenum, the first part of the small intestine. The exact cause of ulcers is
not known. A relationship between smoking cigarettes and ulcers, especially
duodenal ulcers, does exist. The 1989 Surgeon General's report stated that
ulcers are more likely to occur, less likely to heal, and more likely to cause
death in smokers than in nonsmokers.
Why is this so? Doctors are not really sure, but smoking does seem to be one of
several factors that work together to promote the formation of ulcers.
For example, some research suggests that smoking might increase a person's risk of infection with the bacterium Helicobacter pylori (H. pylori). Most peptic ulcers are caused by this bacterium.
Stomach acid is also important in producing ulcers. Normally, most of this acid is buffered by the food we eat. Most of the unbuffered acid that enters the duodenum is quickly neutralized by sodium bicarbonate, a naturally occurring alkali produced by the pancreas. Some studies show that smoking reduces the bicarbonate produced by the pancreas, interfering with the neutralization of acid in the duodenum. Other studies suggest that chronic cigarette smoking may increase the amount of acid secreted by the stomach.
Whatever causes the link between smoking and ulcers, two points have been repeatedly demonstrated: People who smoke are more likely to develop an ulcer, especially a duodenal ulcer, and ulcers are less likely to heal quickly among smokers in response to otherwise effective treatment. This research tracing the relationship between smoking and ulcers strongly suggests that a person with an ulcer should stop smoking.
Liver Disease
The liver is an important organ that has many tasks. Among other things, the liver is responsible for processing drugs, alcohol, and other toxins to remove them from the body. There is evidence that smoking alters the ability of the liver to handle these substances. In some cases, this may influence the dose of medication necessary to treat an illness. Some research also suggests that smoking can aggravate the course of liver disease caused by excessive alcohol intake.
Crohn's Disease Crohn's disease causes inflammation deep in the lining of
the intestine. The disease, which causes pain and diarrhea, usually affects the
small intestine, but it can occur anywhere in the digestive tract. Research
shows that current and former smokers have a higher risk of developing Crohn's
disease than nonsmokers do. Among people with the disease, smoking is
associated with a higher rate of relapse, repeat surgery, and immunosuppressive
treatment. In all areas, the risk for women, whether current or former smokers,
is slightly higher than for men. Why smoking increases the risk of Crohn's
disease is unknown, but some theories suggest that smoking might lower the
intestine's defenses, decrease blood flow to the intestines, or cause immune
system changes that result in inflammation.
Gallstones Several studies suggest that smoking may increase the risk of
developing gallstones and that the risk may be higher for women. However,
research results on this topic are not consistent, and more study is needed.
Can the Damage be Reversed?
Some of the effects of smoking on the digestive system appear to be of short duration. For example, the effect of smoking on bicarbonate production by the pancreas does not appear to last. Within a half-hour after smoking, the production of bicarbonate returns to normal. The effects of smoking on how the liver handles drugs also disappear when a person stops smoking. However, people who no longer smoke still remain at risk for Crohn's disease. Clearly, this question needs more study.
Tobacco related diseases claim approximately 419,000 American lives each year.
Some of the adverse health effects include:
- Cigarettes contain at least 43 individual cancer-causing chemicals and smoking is directly responsible for almost 90% of all lung cancers.
- Smoking causes most of the cases of emphysema and chronic bronchitis.
- Smoking during pregnancy accounts for 20 - 30% of low birthweight infants and up to 14% of preterm births. Approximately 10% of all infant deaths are attributable to smoking.
- Apparently healthy, full-term infants of smokers have been found to be born with narrowed airways and impaired lung function.
- Smoking by parents (second hand smoke) is associated with adverse effects in their children such as exacerbations of asthma, increased upper respiratory infections (colds, ear infections, etc.) and SIDS (sudden infant death syndrome). Children under 18 months of age are very susceptible to secondhand smoke causing lower respiratory tract infections.
- Secondhand smoke is
responsible for 3,000 lung cancer deaths annually in
- Nicotine is a very addictive substance. It reaches the brain faster than drugs that are used intravenously. Users of nicotine become physically, as well as, psychologically addicted. Because nicotine is used socially, this makes it an even more difficult habit to break.
Questions and Answers About Cigar Smoking and Cancer
What are the health risks associated with cigar smoking?
Scientific evidence has shown that cancers of the oral cavity (lip,
tongue, mouth, and throat), larynx, lung, and esophagus are associated with
cigar smoking. Furthermore, evidence strongly suggests a link between cigar
smoking and cancer of the pancreas. In addition, daily cigar smokers, particularly
those who inhale, are at increased risk for developing heart and lung disease.
Like cigarette smoking, the risks from cigar smoking increase with increased
exposure. For example, compared with someone who has never smoked, smoking only
one to two cigars per day doubles the risk for oral and esophageal cancers.
Smoking
The health risks associated with occasional cigar smoking (less than daily) are
not known. About three-quarters of cigar smokers are occasional smokers.
What is the effect of inhalation on disease risk?
One of the major differences between cigar and cigarette smoking is the degree of inhalation. Almost all cigarette smokers report inhaling while the majority of cigar smokers do not because cigar smoke is generally more irritating. However, cigar smokers who have a history of cigarette smoking are more likely to inhale cigar smoke. Cigar smokers experience higher rates of lung cancer, coronary heart disease, and chronic obstructive lung disease than nonsmokers, but not as high as the rates for cigarette smokers. These lower rates for cigar smokers are probably related to reduced inhalation.
How are cigars and cigarettes different?
Cigars and cigarettes differ in both size and the type of tobacco used.
Cigarettes are generally more uniform in size and contain less than 1 gram of
tobacco each. Cigars, on the other hand, can vary in size and shape and can
measure more than 7 inches in length. Large cigars typically contain between 5
and 17 grams of tobacco. It is not unusual for some premium cigars to contain
the tobacco equivalent of an entire pack of cigarettes.
How are the health risks associated with cigar
smoking different from those associated with smoking cigarettes?
Health risks associated with both cigars and cigarettes are strongly
linked to the degree of smoke exposure. Since smoke from cigars and cigarettes
are composed of many of the same toxic and carcinogenic (cancer causing)
compounds, the differences in health risks appear to be related to differences
in daily use and level of inhalation.
Most cigarette smokers smoke every day and inhale. In contrast, as many as
three-quarters of cigar smokers smoke only occasionally, and the majority do
not inhale.
All cigar and cigarette smokers, whether or not they inhale, directly expose
the lips, mouth, tongue, throat, and larynx to smoke and its carcinogens.
Holding an unlit cigar between the lips also exposes these areas to
carcinogens. In addition, when saliva containing smoke constituents is
swallowed, the esophagus is exposed to carcinogens. These exposures probably
account for the fact that oral and esophageal cancer risks are similar among
cigar smokers and cigarette smokers.
Cancer of the larynx occurs at lower rates among cigar smokers who do not
inhale than among cigarette smokers. Lung cancer risk among daily cigar smokers
who do not inhale is double that of nonsmokers, but significantly less than the
risk for cigarette smokers. However, the lung cancer risk from moderately
inhaling smoke from five cigars a day is comparable to the risk from smoking up
to one pack of cigarettes a day.
What are the hazards for nonsmokers exposed to cigar smoke?
Environmental tobacco smoke (ETS), also known as secondhand or passive
smoke, is the smoke released from a lit cigar or cigarette. The ETS from cigars
and cigarettes contains many of the same toxins and irritants (such as carbon
monoxide, nicotine, hydrogen cyanide, and ammonia), as well as a number of
known carcinogens (such as benzene, nitrosamines, vinyl chloride, arsenic, and
hydrocarbons). Because cigars contain greater amounts of tobacco than
cigarettes, they produce greater amounts of ETS.
There are, however, some differences between cigar and cigarette smoke due to
the different ways cigars and cigarettes are made. Cigars go through a long
aging and fermentation process. During the fermentation process, high
concentrations of carcinogenic compounds are produced. These compounds are
released when a cigar is smoked. Also, cigar wrappers are less porous than
cigarette wrappers. The nonporous cigar wrapper makes the burning of cigar
tobacco less complete than cigarette tobacco. As a result, compared with
cigarette smoke, the concentrations of toxins and irritants are higher in cigar
smoke.
In addition, the larger size of most cigars (more tobacco) and longer smoking
time produces higher exposures to nonsmokers of many toxic compounds (including
carbon monoxide, hydrocarbons, ammonia, cadmium, and other substances) than a
cigarette. For example, measurements of the carbon monoxide (CO) concentration
at a cigar party and a cigar banquet in a restaurant showed indoor CO levels
comparable to those measured on a crowded
Are cigars addictive?
Nicotine is the agent in tobacco that is capable of causing addiction or
dependence. Cigarettes have an average total nicotine content of about 8.4
milligrams, while many popular brands of cigars will contain between 100 and
200 milligrams, or as many as 444 milligrams of nicotine.
As with cigarette smoking, when cigar smokers inhale, nicotine is absorbed
rapidly. However, because of the composition of cigar smoke and the tendency of
cigar smokers not to inhale, the nicotine is absorbed predominantly through the
lining of the mouth rather than in the lung. It is important to note that
nicotine absorbed through the lining of the mouth is capable of forming a
powerful addiction, as demonstrated by the large number of people addicted to
smokeless tobacco. Both inhaled and noninhaled nicotine can be addictive. The
infrequent use by the average cigar smoker, low number of cigars smoked per
day, and lower rates of inhalation compared with cigarette smokers have led
some to suggest that cigar smokers may be less likely to be dependent than
cigarette smokers.
Addiction studies of cigarettes and spit tobacco show that addiction to
nicotine occurs almost exclusively during adolescence and young adulthood when
young people begin using these tobacco products. Also, several studies raise
the concern that use of cigars may predispose individuals to the use of
cigarettes. A recent survey showed that the relapse rate of former cigarette
smokers who smoked cigars was twice as great as the relapse rate of former
cigarette smokers who did not smoke cigars. The study also observed that cigar smokers
were more than twice as likely to take up cigarette smoking for the first time
than people who never smoked cigars.
What are the benefits of quitting?
There are many health benefits to quitting cigar smoking. The likelihood of developing cancer decreases. Also, when someone quits, an improvement in health is seen almost immediately. For example, blood pressure, pulse rate, and breathing patterns start returning to normal soon after quitting. People who quit will also see an improvement in their overall quality of life. People who decide to quit have many options available to them. Some people choose to quit all at once. Other options gaining popularity in this country are nicotine replacement products, such as patches, gum, and nasal sprays. If considering quitting, ask your doctor to recommend a plan that could best suit you and your lifestyle.
What are the current trends in cigar smoking?
Although cigar smoking occurs primarily among males between the ages of
35 and 64 who have higher educational backgrounds and incomes, recent studies
suggest new trends. Most new cigar users today are teenagers and young adult
males (ages 18 to 24) who smoke occasionally (less than daily). According to
two large statewide studies conducted among
How are current trends in cigar smoking different from past decades?
Total cigar consumption declined by about 66 percent from 1973 until 1993. Cigar use has increased more than 50 percent since 1993. The increase in cigar use in the early 1990s coincided with an increase in promotional media activities for cigars.
What additional information is available about the effects of cigar smoking?
The 1998 NCI monograph Cigars: Health Effects and Trends can be ordered
from the Cancer Information Service (see below).
Additional information on the health effects of tobacco is available from the
CDC's Tobacco Information and Prevention Source (TIPS) at http://www.cdc.gov/tobacco on the
Internet. This program collects and distributes reports and news about tobacco,
lists services available for people trying to quit using tobacco products, and
produces publications about tobacco and the dangers of its use.
Antidepressants Help Smokers' Hearts
Some antidepressants may do double duty for people who smoke. A study
published in the American Heart Association journal Circulation finds that
selective serotonin reuptake inhibitors may significantly cut smokers' risk for
heart attacks. Researchers from the
Why Do Smokers Fail to Quit?
Although over a quarter of American adults continue to smoke, about 70% of them want to quit. Unfortunately, in one study of women smokers who said they wanted to stop smoking, 80% of them were unable to. Withdrawal is a difficult process. Even after years of not smoking, about 20% of ex-smokers still have occasional cravings for cigarettes. People who keep trying, however, have a fifty-fifty chance of finally quitting. In any case, the attempts to quit are never a waste of time, since the amount of smoking is reduced during these periods. The smoker is up against an army of obstacles to quitting.
Individual Risk Factors for Failure
Researchers have been trying to discover individual risk factors or sets of behaviors that can help predict why specific people fail to quit. Some factors include:
- Being female
- Being a heavy smoker
- Inhaling deeply
- Being a long term smoker
- Severe withdrawal symptoms
Among many studies, however, only one found a single consistent factor for
failure to quit:
Cheating during the first two weeks of withdrawal, even with the patch, nearly
guarantees smoking again in six months. (In one study, nearly half of the
people who did not cheat during the first two weeks were still not smoking
after six months.)
Addictive Aspects of Nicotine
Nicotine is a psychoactive drug, and some researchers feel it is as addictive
as heroin. In fact, nicotine has actions similar to cocaine and heroin in the
same area of the brain.
Depending on the amount taken in, nicotine can act as either a stimulant or a
sedative. Cigarette smoking (either the nicotine or the oral process of smoking
itself) has definite immediate positive effects:
- It relieves minor depression.
- It helps suppress little fits of anger.
- It enhances concentration and short-term memory.
- It produces a modest sense of well-being.
The addictive process of smoking has a specific daily cycle:
Most smokers have a special fondness for the first cigarette of the day because
of the way brain cells respond to the day's first nicotine rush. Nicotine,
particularly taken in first few cigarettes of the day, increases the activity
of dopamine, a chemical in the brain that elicits pleasurable sensations, a
feeling similar to achieving a reward.
During the day, however, the nerve cells become desensitized to nicotine;
smoking becomes less pleasurable, and smokers may be likely to increase their
intake to get their "reward." A smoker develops tolerance to these
effects very quickly and requires increasingly higher levels of nicotine.
Withdrawal in the First Two Weeks
Because the first two weeks are so critical in determining quitting failure
rates, smokers should not be shy about seeking all the help they can during
this period.
Withdrawal symptoms begin as soon as four hours after the last cigarette,
generally peak in intensity at three to five days, and disappear after two
weeks. They include both physical and mental symptoms.
Physical Symptoms. During the quitting process people should consider the following
physical symptoms of withdrawal as they were recuperating from a disease and
treat them accordingly as they would any physical symptoms:
- Tingling in the hands and feet
- Sweating
- Intestinal disorders (cramps, nausea)
- Headache
- Cold symptoms as the lungs begin to clear (sore throats, coughing, and other signs of colds and respiratory problem)
- Mental and Emotional Symptoms.
Tension and craving build up during periods of withdrawal, sometimes to a
nearly intolerable point. One European study found that the incidence of
workplace accidents increases on No Smoking Day, a day in which up to 2 million
smokers either reduce the amount they smoke or abstain altogether.
Nearly every moderate to heavy smoker experiences more than one of the
following strong emotional and mental responses to withdrawal.
- Feelings of being an infant: temper tantrums, intense needs, feelings of dependency, a state of near paralysis.
- Insomnia
- Mental confusion
- Vagueness
- Irritability
- Anxiety
- Depression is common in the short and long term. In the short term it may mimic the feelings of grief felt when a loved one is lost. As foolish as it sounds, a smoker should plan on a period of actual mourning in order to get through the early withdrawal depression.
- Long-Term Depression
There is a significant association between cigarette smoking and a
susceptibility to depression. People who are prone to depression face a 25%
chance of triggering depression when they quit smoking. And, depressed smokers
have a very low level of success; only about 6% remain smoke-free after a year.
There are strong reasons for this:
Smoking may be masking major depression, which can become severe even after the
early stages of withdrawal have passed.
For some smokers, the future physical damage incurred by smoking is an
abstraction, which fails to motivate quitting when measured up against the very
real emotional pain triggered by nicotine withdrawal.
Not only does the smoker suffer, but the negative emotions often harm relationships
with friends and family, who might even urge the ex-smoker to take up
cigarettes again.
People who suffer from depression associated with quitting might do better
using a combination of emotionally supportive therapy (as opposed to behavioral
therapy), nicotine replacements, and temporary use of antidepressants, such as
bupropion (Zyban). If severe depression lasts beyond withdrawal, professional
help should be sought as soon as possible.
Advertising as Reinforcement
Advertising reinforces the addiction by presenting smokers as ideal adults,
people who have outgoing cheerful attitudes, are able to work and play
exuberantly, are often risk-takers, and enjoy the present moment. This
insidious message is doubly attractive to a smoker who is trying to quit; the
withdrawal state puts one in an emotionally infantile state. The ads remind the
smoker that, with the purchase of a pack of cigarettes, it's very easy to
become a grown-up again. (And, even worse, these same ads are telling children
that smoking is a short cut to adulthood.)
Weight Gain
The emphasis on weight loss in our society has given many people an excuse to
start or continue smoking.
Effects of Smoking on Calories. Smoking does indeed use up calories, about 200
a day according to one study. A 1999 study reported that smoking increases
energy expenditure in men by 3.6% at rest and by 6.3% during physical activity.
(Actually, the higher level during exercise was only because the men inhaled
more deeply during that time.)
Reasons for Weight Gain after Quitting. Quitting can add five or more pounds,
due to the following reasons:
- Obviously, the body is working better. After quitting, the body's metabolism slows down, and food is digested more efficiently.
- Insulin levels increase, enabling the body to process more sugar for energy.
- People snack as an oral substitution.
- Long-Term Effects of Abstinence on Weight. One 1998 study reported that people who quit smoking put on more weight than expected, and although they gained most of the weight in the first year, they kept adding weight over a period of five years. This contradicts other studies that ex-smokers lost their extra weight over a year or two and that the longer they abstained from smoking the more weight they lost. Indeed, an encouraging 1999 study reported that weight gain tends to peak between two and four years after quitting and then declines to the same rate as those who never smoked.
Keeping the Weight Off. It should be noted that to use up the 200 calories gained
from quitting smoking, one need only take an extra 15-minute daily walk and
eliminate 100 calories a day from meals. Even a moderate increase in physical
activity among middle-aged women who have quit smoking can help keep weight
gain to a minimum. (Using Zyban also appears to help protect against weight
gain.)
RECENT LITERATURE
Development of major depression after treatment for smoking cessation. Am J
Psychiatry. 2000 Mar;157(3):368-74.
ABOUT WELL-CONNECTED
Well-Connected reports are written and updated by experienced medical writers
and reviewed and edited by the in-house editors and a board of physicians,
including faculty at Harvard Medical School and Massachusetts General Hospital.
The reports are distinguished from other information sources available to
patients and health care consumers by their quality, detail of information, and
currency. These reports are not intended as a substitute for medical
professional help or advice but are to be used only as an aid in understanding
current medical knowledge. A physician should always be consulted for any
health problem or medical condition.
This report may not be copied, displayed on Internet web sites, or otherwise
distributed without the express permission of the
'Light' Cigarettes Burned by Tobacco Control Advocates
No Evidence to Indicate the Risk Is Lower
By Sean Martin
WebMD Washington Correspondent
Reviewed by Dr. Jacqueline Brooks
"Light" or "mild" cigarettes provide little real health
benefits over regular brands, tobacco control advocates maintained Monday at
the 11th World Conference on Tobacco OR Health.
"Low-yield" brands with reduced nicotine and tar levels have grown in
popularity since the late 1960s to take up about two-thirds of the U.S.
cigarette market. This growth has been spurred by increasing health concerns
over cigarettes. But anti-tobacco leaders worry that these brands give smokers
a false impression of being less harmful.
William Farone, an industry "whistleblower" as former director of
applied research at Philip Morris, tells WebMD, "I don't think people
generally understand that smoking a low-cigarette isn't safer."
In a presentation Monday, David Burns, MD, of the University of California at
San Diego School of Medicine, said, "The evidence does not suggest that a
meaningful reduction in risk has been produced by shifting to low-yield
cigarettes."
Gregory Connolly, director of the Massachusetts Tobacco Control Program, tells
WebMD, "The evidence would show, in fact, that they are as harmful as
conventional cigarettes." According to Ann McNeill, PhD, a public health
consultant, low-yield cigarettes have brought "little, if any,
benefit" to public health and possible health harm to the degree that they
have kept smokers from quitting altogether.
Lung cancer is still the leading cancer among U.S. men, and in 1987 it began
outpacing breast cancer among American women.
Farone noted that internal documents have revealed that the tobacco industry
has long been aware that people who smoke lighter cigarettes often compensate
for lower nicotine levels by smoking more cigarettes. In addition, he said,
these smokers might draw smoke more deeply into their lungs, triggering
different types of lung cancer.
According to Farone, a lighter cigarette "still has all the [cancer-causing
agents], and maybe even more." Regardless of its nicotine and tar levels,
tobacco smoke contains carbon monoxide and cancer-causing nitrosamines.
Moreover, tobacco firms use a large list of additives in cigarettes that have
unknown health effects.
European Union health ministers have approved guidelines that outlaw brands
being marketed as light or mild. Peter Boyle, a researcher from Italy's
European Institute of Oncology, reported results that found a ninefold
difference among 29 countries in nitrosamine levels in cigarettes. He and many
other tobacco control advocates believe that cigarettes should be regulated for
levels of the cancer-causing compound.
That may be a long time coming in the U.S., where cigarettes and their
component ingredients are not strictly controlled, and the Supreme Court ruled
earlier this year that the FDA lacks the authority to regulate cigarettes.
Clifford Douglas, a tobacco control consultant, tells WebMD, "That
[government] oversight is essential. Otherwise, we've got an industry
self-regulating under a very imperfect system of public pressure and individual
states." Congress may take action next year to regulate tobacco in some
way, but the tobacco industry holds impressive clout with many lawmakers.
Meanwhile, Connolly is trying to get Massachusetts to set state regulatory
standards for cigarettes based on their toxicity and addictiveness.
He tells WebMD, "If Jesse Helms wants kids smoking Marlboro Light 100s in
North Carolina, that's fine with us." He notes that before his state can
act, however, "We still have four active lawsuits against us."
As for the industry, RJ Reynolds is test-marketing the Eclipse cigarette, which
heats tobacco rather than burns it and may reduce some of a cigarette's
toxicity.
Tobacco industry representatives have not been invited to this meeting, but
organizers said that they were free to register and have attended past
meetings.
YOU CAN QUIT SMOKING
(A consumer guide from the U.S. Department of Health and Human Services
Public Health Services)
NICOTINE: A POWERFUL ADDICTION
If you have tried to quit smoking, you know how hard it can be. It is hard
because nicotine is a very addictive drug. For some people, it can be as
addictive as heroin or cocaine.
Quitting is hard. Usually people make 2 or 3 tries, or more, before finally
being able to quit. Each time you try to quit, you can learn about what helps
and what hurts.
PURPOSE OF THIS BOOKLET
This booklet tells about ways you can get help to quit smoking. It explains the
best ways for you to quit, and quit for good. All the information in this
booklet is based on scientific research about what will give you the best
chances of quitting. The booklet also lists names and addresses of
organizations that can offer help and more information.
QUITTING TAKES HARD WORK AND A LOT OF EFFORT, BUT—YOU CAN QUIT SMOKING.
GOOD REASONS FOR QUITTING
Quitting smoking is one of the most important things you will ever do:
You will live longer and live better. Quitting will lower your chance of having
a heart attack, stroke, or cancer. If you are pregnant, quitting smoking will
improve your chances of having a healthy baby. The people you live with,
especially your children, will be healthier. You will have extra money to spend
on things other than cigarettes.
FIVE KEYS FOR QUITTING
Studies have shown that these five steps will help you quit and quit
for good. You have the best chances of quitting if you use them
1. Get ready.
2. Get support.
3. Learn new skills and behaviors.
4. Get medication and use it correctly.
5. Be prepared for relapse or difficult situations.
1. GET READY
Set a quit date.
Change your environment.
— Get rid of ALL cigarettes and ashtrays in your home, car, and place of
work.
— Don’t let people smoke in your home.
Review your past attempts to quit. Think about what worked and what did not.
Once you quit, don’t smoke—NOT EVEN A PUFF!
2. GET SUPPORT AND ENCOURAGEMENT
Studies have shown that you have a better chance of being successful if you
have help. You can get support in many ways:
Tell your family, friends, and coworkers that you are going to quit and want
their support. Ask them not to smoke around you or leave cigarettes out.
Talk to your health care provider (for example, doctor, dentist, nurse,
pharmacist, psychologist, or smoking counselor).
Get individual, group, or telephone counseling. The more counseling you have,
the better your chances are of quitting. Programs are given at local hospitals
and health centers. Call your local health department for information about
programs in your area.
3. LEARN NEW SKILLS AND BEHAVIORS
Try to distract yourself from urges to smoke. Talk to someone, go for a walk,
or get busy with a task.
When you first try to quit, change your routine. Use a different route to work.
Drink tea instead of coffee. Eat breakfast in a different place.
Do something to reduce your stress. Take a hot bath, exercise, or read a book.
Plan something enjoyable to do every day.
Drink a lot of water and other fluids.
4. GET MEDICATION AND USE IT CORRECTLY
Medications can help you stop smoking and lessen the urge to smoke.
The U.S. Food and Drug Administration (FDA) has approved five medications to
help you quit smoking:
— Bupropion SR - available by prescription
— Nicotine gum - available over-the-counter
— Nicotine inhaler - available by prescription
— Nicotine nasal spray - available by prescription
Nicotine patch - available by prescription and over-the-counter
Ask your health care provider for advice and carefully read the information on
the package.
All of these medications will more or less double your chances of quitting and
quitting for good.
Everyone who is trying to quit may benefit from using a medication. If you are
pregnant or trying to become pregnant, nursing, under age 18, smoking fewer
than 10 cigarettes per day, or have a medical condition, talk to your doctor or
other health care provider before taking medications.
5. BE PREPARED FOR RELAPSE OR DIFFICULT SITUATIONS
Most relapses occur within the first 3 months after quitting. Don’t be
discouraged if you start smoking again. Remember, most people try several times
before they finally quit. Here are some difficult situations to watch for.
Alcohol. Avoid drinking alcohol. Drinking lowers your chances of success.
Other smokers. Being around smoking can make you want to smoke.
Weight gain. Many smokers will gain weight when they quit, usually less than 10
pounds. Eat a healthy diet and stay active. Don’t let weight gain
distract you from your main goal—quitting smoking. Some quit-smoking
medications may help delay weight gain.
Bad mood or depression. There are a lot of ways to improve your mood other than
smoking.
If you are having problems with any of these situations, talk to your doctor or
other health care provider.
SPECIAL SITUATIONS OR CONDITIONS
Studies suggest that everyone can quit smoking. Your situation or condition can
give you a special reason to quit.
Pregnant women/new mothers: By quitting, you protect your baby’s health
and your own.
Hospitalized patients: By quitting, you reduce health problems and help
healing.
Heart attack patients: By quitting, you reduce your risk of a second heart
attack.
Lung, head, and neck cancer patients: By quitting, you reduce your chance of a
second cancer.
Parents of children and adolescents: By quitting, you protect your children and
adolescents from illnesses caused by second-hand smoke.
QUESTIONS TO THINK ABOUT
Think about the following questions before you try to stop smoking. You may
want to talk about your answers with your health care provider.
Why do you want to quit?
When you tried to quit in the past, what helped and what didn’t?
What will be the most difficult situations for you after you quit? How will you
plan to handle them?
Who can help you through the tough times? Your family? Friends? Health care
provider?
What pleasures do you get from smoking? What ways can you still get pleasure if
you quit?
Here are some questions to ask your health care provider.
How can you help me to be successful at quitting?
What medication do you think would be best for me and how should I take it?
What should I do if I need more help?
What is smoking withdrawal like? How can I get information on withdrawal?
FOR MORE INFORMATION
For information about the guideline or to get more copies of this booklet, call
toll free: 800-358-9295, or write:
Publications Clearinghouse
P.O. Box 8547
Silver Spring, MD 20907
QUITTING TAKES HARD WORK AND A LOT OF EFFORT, BUT—YOU CAN QUIT SMOKING!!
Tobacco Regulations Clouded
The Supreme Court has to consider both historical precedent and the balance
of power among government agencies.
By Randy Wilson , JD
The Supreme Court has to consider both historical precedent and the balance of
power among government agencies. Earlier this month, the court heard arguments
from both government and tobacco attorneys regarding whether the FDA had the
authority to regulate cigarettes. A lower court, the 4th U.S. Circuit Court of
Appeals, ruled last year that the FDA cannot regulate cigarettes. Supreme Court
justices, in early review, appear to be leaning toward upholding that
lower-court ruling.
How can that be? Scientific evidence continues to mount that cigarette smoking
is the greatest public health hazard facing the United States. Popular opinion
strongly favors bans against smoking in public places. Cities such as San
Francisco have banned smoking in restaurants and bars. Why is the Supreme Court
looking at bucking this trend?
Mainly because the FDA's origins lie in regulating medicines, and historically
tobacco has not been included under the agency's purview. The FDA's power to
regulate drugs originated with the Food, Drug, and Cosmetic Act passed by
Congress in 1938. For years, the FDA claimed it did not have the power to
regulate cigarettes -- limiting its mission to ensuring that medical devices,
including drugs, are safe and effective.
In an abrupt turn in 1996 based on new medical evidence that showed the highly
addictive qualities of nicotine, the FDA decided that it should regulate
tobacco. The agency argued that if it had the ability to regulate NoDoz
stay-awake stimulants, for one example, it should have the same right to
regulate nicotine.
However, tobacco lawyers claim there is a big difference between NoDoz, which
is a drug intended to keep people awake, and the nicotine in tobacco, which has
no medical benefit. Tobacco lawyers, calling the government's bluff in a sense,
have also argued that if cigarettes are so dangerous, they should be banned
rather than regulated.
In my opinion, the Supreme Court will have a tough time ruling against the
tobacco industry. If the FDA is allowed to expand its reach in regulating
cigarettes without an act of Congress, it will open the door to allowing other
government agencies to stretch their authority as well. This would be a
dangerous precedent, possibly undermining the checks and balances built into
our system of government.
That said, this case provides the Supreme Court with an opportunity to force
Congress to face a glaring public-policy conflict. Congress has subsidized the
tobacco industry, encouraging the production of a deadly consumer product,
while at the same time attempting to curtail the sale of that product. If the
Supreme Court rules against the FDA, Congress and the nation will have to debate
how to handle the production and sale of cigarettes in the United States.
2000 Healtheon/WebMD. All rights reserved.
Fighting Against a Mass Murderer
Lung cancer is America's leading cancer killer. Women who smoke seem
especially resistant to the message. By Beatrice Motamedi
WebMD Medical News
Reviewed by Dr. Craig H. Kliger
Feb. 26, 2001 -- Michelle Globerson started smoking when she was just 15 years
old. Now 45, she's quit smoking four times, each time cold turkey, but never
for good.
Recently, she's been seeing more and more public service announcements on TV,
including one spot that calls smoking "puking (and) disgusting." She
agrees. But she's still not ready to give up her pack-a-day habit.
"I know it's wrong -- I'm hurting myself," says Globerson, a
supervisor for a pool building company in Mesa, Ariz. "Something is going
to make me want to quit. I just don't know what it will be."
She has plenty of company. Despite a decline in U.S. smoking rates since the
mid-1960s, tobacco use among women remains stubbornly high.
At first glance, the nationwide numbers seem to favor females. Just 20.9% of
adult women smoke, compared with 24.2% of men, according to the latest CDC
data. But the data mask a remarkable drop of nearly 47% in male smoking rates
between 1965 and 1995, compared to a more modest decline of 35% for women.
More worrisome is the increase in lung cancer cases. Among women, they've more
than doubled since 1973, according to the American Lung Association. Lung
cancer mortality fell by 3.2% for men between 1992 and 1997, but among women
the rate was essentially unchanged.
There's also concern about teens. While youth smoking rates appear to have
steadied after years of increases, an important new study raises serious
questions about the effectiveness of school-based programs, a mainstay of teen
education efforts.
The study, by researchers at the Fred Hutchinson Cancer Research Center in
Seattle, appeared in the December 2000 issue of the Journal of the National
Cancer Institute. It surveyed smoking rates among 8,400 students in Washington
state, half of whom had been exposed to an intensive, grade 3-to-12 program.
The program was based on the popular "social influences" approach,
which teaches kids how to resist TV ads and peer pressure through media
literacy classes, role-playing, and other behavioral exercises.
The results were surprising: Researchers found "no significant
difference" in tobacco use between students who had gone through the
program and those who hadn't; the smoking rate among 12th grade girls who took
antismoking classes, for example, was 24.4%, compared with 24.7% for those who
didn't.
"It was disappointing, because the social influences approach has been
such an attractive one," says Arthur V. Peterson Jr., PhD, a Hutchinson
researcher and professor of biostatistics at the University of Washington.
"We had high hopes."
A leading cause of cancer deaths
Lung cancer is America's No. 1 cancer killer, claiming more lives than any
other type. The CDC estimates that 164,100 new cases were diagnosed last year;
each year, more than 156,900 men and women die from lung cancer, representing
nearly 28% of all cancer deaths.
Perhaps the only good thing about lung cancer is that the usual cause is easy
to identify: cigarette smoking, which causes up to 90% of all such cases,
according to the National Cancer Institute (NCI).
Increasingly, states such as Arizona, California, Oregon, Massachusetts, and
Florida have turned to public service ads, clean air laws, and taxes on
cigarettes, in their bids to drive down smoking and cancer rates. Last year saw
the debut of more statewide tobacco control laws than ever before, according to
the American Lung Association, including 113 new laws in 43 states.
Controversial and costly as they may be, evidence indicates that tobacco
control programs work, particularly for women. California, which launched its
program in 1988, saw smoking drop from 22.4% to 18% between 1988 and 1997,
according to a December report by the CDC. Lung cancer cases plunged by 14%,
compared to a decline of 2.7% in a sample that included five states and three
cities. Among women, the impact was even more striking: A 4.8% drop in lung
cancer incidence within California, compared with an increase of 13.2% elsewhere.
Critics point out that smoking rates were already on their way down by the time
California took aim at tobacco. "But the rate of decline has accelerated
-- it's two to three times as rapid as the declines around the country,"
says Terry Pechacek, PhD, associate director for science in the CDC's Office of
Smoking and Health.
And while it will take 10 to 15 years to see the full effect of lower smoking
on lung cancer, heart disease is another story: "More than half [of the
risk] is gone within one or two years of quitting," Pechacek says. Heart
disease is the leading cause of death among women; lung cancer is second.
TV, taxes and treatment
Experts agree that what makes the California model work is that it's
comprehensive and doesn't rely on any one approach, a lesson hammered home in
the Hutchinson study.
Creative as it was -- 10th graders even re-enacted testimony given by tobacco
executives before Congress, just to get a sense of the issues -- the Hutchinson
program provided kids with a total of just 46.75 hours of instruction over nine
years of schooling. Compare that, Peterson says, to the estimated $7 billion
spent each year by tobacco companies on advertising and marketing.
"It's like a raft on a raging sea," Peterson says, of school-based
education. "From the results of this study, we would conclude that this
raft has no chance. So more and different things must be done."
What should they be? Increasingly, states are turning to a triad of TV ads, taxes, and treatment.
In California, Arizona, Florida, and Massachusetts, aggressive TV and print
campaigns portray smoking not only as unhealthy but uncool. In Florida, TV
spots crafted with the help of teens hit hard at tobacco companies, with ads
that featured images of corrupt executives and corpses in body bags. Edgy and
sometimes gritty, the ad campaign, called "Truth," is credited with a
40% reduction in teen smoking between 1998 and 2000.
Taxes on tobacco are another strategy: Over the past decade, all 50 states have
adopted them, from a high of $1 per pack in Alaska to 35 cents in Nevada. Some
suggest they could be raised even more.
Youth smokers "are somewhere between two and four times as
responsive" to price hikes as adults, says David Levy, PhD, senior
scientist at the Pacific Institute for Research and Evaluation in Rockville,
Md., and a professor of economics at the University of Baltimore.
African-American adolescents are particularly sensitive to price swings, he
says.
That fact alone could be a powerful weapon: A study in the December 2000 issue
of the Journal of the National Medical Association reported that black
teenagers who smoke are more likely to develop lung cancer and other long-term
problems, even though black teens as a group smoke less than their white peers.
Researchers believe racial differences in the way nicotine is metabolized could
make tobacco more lethal for blacks.
"You could say it's regressive," says Levy, of taxes that
disproportionately affect black youth. "But death is regressive."
Improving treatment options is the third approach. For many smokers, the worst
thing about quitting is that it's expensive; the CDC estimates that it can cost
as much as $400 for a three-month "quit attempt" using the nicotine
patch. Unfortunately, insurance rarely pays.
Some states may force the issue. In Maryland, a coalition of state officials
and advocacy groups intends to introduce what would be the nation's first law
requiring private insurers to pay for prescription antismoking drugs.
"This is a hard sell, believe me," says Joan Stine, director of
Maryland's Office of Health Promotion, adding that an earlier version of the
bill was torpedoed last year by the state's HMOs.
"In the long run, you save money on these folks if they stop
smoking," Stine says. "But [HMOs] don't operate in the long
run."
Not quitting, but still watching
One reason for the focus on smoking is that unlike breast or prostate
cancer, there is no widely available, effective screening test for early stage
lung cancer.
Currently, the NCI is in the midst of a yearlong study of 3,000 patients, to
determine whether low-dose CT (computed tomography) scans are safer and more
effective than chest X-rays. Indeed, a review article in the Nov. 30, 2000,
issue of The New England Journal of Medicine cautions against "compromise
or shortcuts in the rigorous scientific process required to determine whether
this practice is justified," finding from their review of literature to
date, "there does not appear to be a dramatic impact on survival."
They further note: "Too often, presumed solutions prematurely become
standard medical care before the appropriate studies have been completed."
So prevention remains key. For Globerson, that probably means more TV ads. Some
of them make her flinch, but she forces herself to watch.
"Because it does make me think," she says. "Maybe the next time
I see the commercial, that will be the time I stop."
Beatrice Motamedi is a health and medical writer based in Oakland, Calif.,
who has written for Hippocrates, Newsweek, Wired, and many other national
publications.
Why Cigarettes are a Woman's Worst Enemy
Sure, cigarettes can harm anybody, men and women alike. But some of
smoking's ill effects, from ectopic pregnancy to premature menopause, are
reserved for women only. This November 19 is the American Cancer Society's 22nd
Great American Smokeout. If you haven’t decided to give up smoking yet,
here are some compelling reasons to quit now.
By Peg Rosen
Sure, cigarettes can harm anybody, men and women alike. But some of smoking's
ill effects, from ectopic pregnancy to premature menopause, are reserved for
women only. This November 19 is the American Cancer Society's 22nd Great
American Smokeout. If you haven’t decided to give up smoking yet, here
are some compelling reasons to quit now.
Smoking Increases Your Risk of Cervical and Rectal Cancer
Not only can smoking cause a variety of cancers in both men and women, it puts women at higher risk of cervical cancer, according to the American College of Obstetricians and Gynecologists (ACOG). A Danish study published in the April 21, 1999 issue of the Journal of the National Cancer finds that premenopausal women who smoke are six times more likely to develop rectal cancer than those who don't. Smoking Worsens Your Period According to the ACOG, women who smoke experience more severe premenstrual symptoms and have a 50 percent increase in cramps lasting two or more days.
Smoking Damages Your Fertility
Smoking affects practically every phase of conception, according to Vicki Seltzer, M.D., vice president for women’s health services at North Shore-Long Island Jewish Health System in New York. "Smokers have a greater risk of not ovulating, and it is also less likely that a fertilized egg will implant in the uterus. Smokers who receive in vitro fertilization are less likely to be successful." Seltzer also notes that nicotine interferes with the function of the fallopian tube and can hinder an egg from traveling normally to the uterus, which can lead to an ectopic or tubal pregnancy -- potentially life-threatening conditions.
Smoking Hurts Your Unborn Baby
"When you smoke during pregnancy, you poison the fetus," says
Benjamin Sachs, professor of obstetrics and gynecology at Harvard Medical
School. "Carbon monoxide has a greater affinity for fetal tissue than for
adult tissue, and when nicotine crosses the placenta it speeds up the
[baby’s] heart rate."
According to the ACOG, smoking increases a pregnant woman's risk of miscarrying
by 39 percent and heightens the chances of other serious complications,
including placental abruption (when the placenta separates from the uterine
wall), placenta previa (when the placenta covers the opening of the uterus) and
stillbirth.
Many studies have pointed to maternal smoking as the most preventable cause of
low birth weight. The breast milk of smokers can carry nicotine to a suckling
baby. And a 1995 report in the Journal of Pediatrics found that infants exposed
to tobacco smoke are nearly three times more likely to die from sudden infant
death syndrome.
Smoking Ages You
You've probably noticed that smokers develop wrinkles earlier than nonsmokers. What often goes unnoticed is that smoking hastens menopause by one to two years. "Nicotine interferes with the blood supply to the ovary, and if you decrease blood supply to any organ, you decrease its function," says Sandra Carson, M.D., professor of obstetrics and gynecology at Baylor College of Medicine in Houston. Estrogen is produced in the ovaries, which "could explain why smoking brings on earlier menopause," Carson says. Cigarettes can lead to early osteoporosis, too, adds Carson: many studies have shown smoking significantly reduces bone mineral density.
Cigarettes Go to Your Heart
A woman who smokes is two to six times more likely to have a heart attack than one who doesn't, according to the National Institutes of Health. One to four cigarettes a day is enough to double your risk of heart disease, says the ACOG. And a Finnish study published in the July 1998 British Medical Journal found that female smokers are twice as likely to have a heart attack after age 65 as male smokers. Researchers believe estrogen -- which smoking apparently inhibits -- helps protect women against heart disease.
And remember that your behavior sets an example for your daughter or any girl
in your life. "The rate of high school girls who are smoking is now on par
with that of boys," says Wanda Jones, a spokeswoman for the National
Women’s Health Information Center. "This is not the kind of equality
for women our mothers and grandmothers envisioned."
Limits on Teen Cigar Sales: Just Blowing Smoke?
Study Shows Minors Can Make Purchases on the Internet
By Gay Frankenfield, RN
WebMD Medical News
The sale of tobacco products to minors is illegal in the U.S., but that doesn't
mean it doesn't happen. Age disclosure is often not required to purchase cigars
on the Internet, according to a report in the May issue of the American Journal
of Public Health.
"The findings are concerning in light of a 1997 study that showed 22% of
high school students smoked a cigar in the previous month," says study
author Ruth Malone, RN, PhD, an assistant professor of nursing and health
policy at the University of California at San Francisco.
As if looking to purchase cigars, Malone searched the web for cigar links and
visited 140 sites in 1998. Each site was then analyzed for legal and health
warnings, payment terms, and promotional strategies. To assess recent trends, a
second search for cigar links was conducted in 1999, Malone says.
Only 25% of the sites included a statement prohibiting tobacco sales to minors
and just 10 sites required age disclosure prior to purchase. In addition to
credit cards, a third of the sites accepted cash on delivery, money orders, and
personal checks. Also, one in three sites used promotional cartoons, which may
appeal to a young audience. Only five sites provided health warnings.
Just one year later, there was a threefold increase in the number of links to
cigar sites. Malone tells WebMD that the increase shows that Internet cigar
sales are likely to continue to grow. "The number of minors on the net is
also expected to increase from 10 to 45 million over the next two years."
Others claim that cigarettes are a much bigger problem among minors. "It's
been shown that 60% of all teen-agers have tried a cigar, but less than 5%
smoked a second cigar," says Marc Schneiderman, MD, president of the
Allegheny Chapter of the Pennsylvania Academy of Family
Physicians. "But there are 3,000 new cigarette smokers every day, most of
which are teen-agers."
Schneiderman, who smokes two cigars a day, conducted a review of cigar research
since 1950. "Inhalation habits and alcohol abuse both appear to play an
important role in the development of tobacco-related diseases," says
Schneiderman. "But many of the studies have methodological flaws that
limit the findings."
Still, the researchers say more efforts are needed to enforce the law. The
Synar Amendment encourages restriction of tobacco sales to minors by limiting
federal monies to states that are not in compliance. "Teen-age sting
operations are used to test compliance," says Malone, "and it may be
a good strategy for the Internet as well."
Referring to a 1998 joint statement on electronic commerce, Malone adds that
the U.S. and Australia agreed to limit children's access to unsuitable Internet
content with filtering and blocking systems. At present, the Clinton
administration continues to look for ways to keep tobacco out of the hands of
children, according to Mark Kitchens, a White House spokesman.
The study was supported with a grant from the National Cancer Institute.
Vital Information:
- Age disclosure is often not required to buy cigars on the Internet, and health warnings are rare.
- Most sites don't issue a statement prohibiting tobacco sales to minors, and many accept forms of payment other than credit cards.
- Public health experts call for strict enforcement of existing laws, including the Synar Amendment that limits federal monies to states that are not in compliance.
Glamorous Image Lights Fire Under Cigar Sales
Public Health Officials Try to Snuff Out Demand
By Jeff Levine
WebMD Washington Bureau Chief
Whether it's a movie star puffing contentedly on a panatela or teen idols
brandishing their stogies in menacing defiance of societal norms, cigars have
come to be increasingly important status symbols for smokers and a growing
concern to public health officials.
Ironically, during a time when doctors and regulators have put extraordinary
efforts into sending out messages about the dangers of cigarettes and chewing
tobacco, cigar sales are smoking. Researchers say premium cigar sales have
increased from 90,000 in 1986 to 274,000 in 1996. That trend has generated a
wave of studies that were presented at the American Public Health Association's
127th annual meeting here this week.
Not surprisingly, a study of cigar advertising over the last decade shows that
it targets men and promotes the power of cigars to attract women and wealth.
Elisabeth Gruskin, DrPH, of the Institute for Health Policy Studies at the
University of California, San Francisco (UCSF), says that the 92 ads she looked
at generally depicted men luxuriating with their cigars in upscale
environments; women were generally portrayed as sexual conquests.
In one example, the message of an advertisement with a woman draped
languorously over a smiling, male cigar smoker makes the point, "When you
only have time for a quickie."
A study done by the Office of Inspector General at the Department of Health and
Human Services suggests the proliferation of pro-cigar messages is getting
through to children. Recent research involving 230 teens was aimed at gaining
an understanding of how children feel about cigar use and its health
consequences.
The information was gathered from junior high school, high school, and college
focus groups. Among the findings, says lead researcher Elise Stein, MPH, are
that about three-fourths of teens report widespread cigar use and
experimentation among their peers. Manufactured cigars, rather than premium
smokes, are most popular. 'Blunting' -- the practice of removing tobacco from a
cigar and spiking it with marijuana -- is said to be widespread.
Stein says her analysis shows that teens believe cigars are more socially desirable
than cigarettes and that they are easy to purchase. Among the issues to be
studied, she says, is the loophole in federal regulations for cigars. They are
exempt from current FDA rules that control tobacco sales because of subtle
technical questions about their addictive properties. In addition, cigars don't
face the same advertising disclosure rules as cigarettes.
Lynn Wenger, MPH, also of the Institute for Health Policy Studies at UCSF,
collected some 600 articles about cigars between 1992 and 1998; they were more
or less evenly divided between general interest and specialty cigar magazines.
The approach varied from the elite Cigar Aficionado to the lower-end, more
youthful Smoke.
But whether the cover featured actor Tom Selleck or rock group Red Hot Chili
Peppers, the message inside was generally uncritical. Wenger says that only 1%
of the articles in cigar magazines focused on health issues related to the
product. Just 3% of cigar-oriented pieces in the other magazines discussed
health matters; most of the pieces discussed cigars as a business.
Both cigar and non-cigar magazines leaned heavily on celebrities in their
product-related pieces.
"The use of cigars is rationalized [as] a fad or a trend," says
Wenger who feels that their needs to be more anti-cigar advocacy in the media.
Still Smoking in 2000? Professional Advice on Medications That Work
Author Linda Hyder Ferry, M.D., M.P.H., discusses how medical assistance can
help you quit smoking.
By Linda Hyder-Ferry , MD, MPH
Moderator: Welcome to WebMD. Today we will be discussing Still Smoking
in 2000? Professional Advice on Medications That Work with Linda Hyder Ferry,
M.D., M.P.H.
Dr. Linda Hyder Ferry is the co-author of the How To Quit Smoking and Not Gain
Weight Cookbook. She is the founder of F.I.N.D. (the Foundation for Innovations
in Nicotine Dependence), an associate professor at the Loma Linda University
School of Medicine, and a leading nicotine-dependence researcher who first
studied the use of bupropion (Zyban) as a nicotine-free treatment for smoking
cessation. She teaches medical students and physicians how to help smokers
optimize their smoke-free futures.
Do smokers really need professional medical assistance to quit smoking? Most
ex-smokers have done it on their own (cold turkey), right?
Dr. Ferry: There are 50 million people who used to smoke in the U.S.
When you ask them how they quit smoking, a significant number will say they did
it on their own. Does that mean it's the best way? Absolutely not. Most people
trying to quit on their own will have to try 5 to 7 times, whereas with
professional medical support, you only need to try once to be successful. What
does that mean? Professional medical assistance? It means someone helps you
assess why you smoke, determines if you have any underlying medical conditions
that make you dependent upon nicotine, and can help you select the correct
medications to help reduce your nicotine withdrawal symptoms and prevent
relapse. Quit rates on your own amount to 5% success rate at the end of the
year. However, professional assisted quit rates are from 40 to 60% at the end
of the year. If you had cancer, would you try to cure it on your own with a 5%
quit rate, or would you rather go for professional help from someone who knows
how to cure cancer? Very very few people who stay abstinent for one year
relapse the second year; 75% of the relapse occurs in the first three, four
months. It drops down to a 10 to 15% quit rate, and then after six months, goes
down to 5%. The majority of the relapse happens very early.
Moderator: What about the over-the-counter herbal stop-smoking agents
that are promoted? Are they proven to work?
Dr. Ferry: Herbal products and non-prescription or over-the-counter
products to stop smoking do not require any trials to prove their effectiveness
prior to marketing.I would encourage caution for any product that says
"guaranteed to work or money back". $29.95. Those are usually money
making scams, and you don't get your money back.Are there no benefits from herbal
products? That can't be stated for sure. Herbal products that change the
chemistry in the brain affecting moods and feelings, may well work similarly to
nicotine in the brain, as it is an "herbal product" from the tobacco
plant. However, it's one manipulated by the tobacco manufacturers. To date, we
have no clinical trials showing that herbal products improve the quit rates
compared to placebo.
Moderator: How does Bupropion Hydrochloride (Zyban) work?
Dr. Ferry: There are two FDA approved medications to control nicotine
withdrawal symptoms during the attempts to quit smoking. Nicotine replacement
therapy (NRT) replaces nicotine in your brain, to keep the smoker from having
nicotine withdrawal symptoms. The non-addicting and nicotine free product
approved in 1997, named buproprian (Zyban), is not a replacement for nicotine.
It is a mood stabilizing modifier of the brain's neurochemistry called an
amino-ketone class.It stabilizes the dopamine and norepinephrine in the brain
that are responsible for the nicotine withdrawal symptoms when someone stops
using tobacco. Those symptoms are irritability, frustration, insomnia, anxiety,
difficulty concentrating, restlessness, increased appetite, and depressed mood.
Zyban is believed to control these symptoms by keeping the levels of
norepinephrine and dopamine stable in someone's brain, instead of having them
bottom out when you quit smoking.
It may have other functions of which we are unaware, but the response of
patients using Zyban in the 1 to 2 weeks before they give up tobacco, and quit
smoking, follows the following pattern. #1, I no longer am enjoying the
pleasure or taste of smoking. #2, I am much calmer now that I am cutting back
on tobacco or have quit. #3, I am no longer experiencing the severe cravings,
and can go for hours without even needing to think to smoke. #4, I am not as
sad, or blue, or bored, or lonely feeling as I usually am when I try to go for
long periods without nicotine. Those responses indicate to me that at least in
the effects of tobacco on these neurotransmitters in a smoker's brain, Zyban is
assisting the smoker to avoid the ups and downs of nicotine withdrawal
symptoms, by some mechanism.
Moderator: How are sugar and insulin involved when a smoker quits?
Dr. Ferry: Nicotine stimulates a variety of neurotransmitters that
affect appetite.
Dr. Ferry: One of them is seretonin.
Dr. Ferry: Seretonin is also known to be related to a carbohydrate binge
that sets off appetite, increasing the desire for sugar or starch. People who
crave carbohydrates may have low seretonin levels, so when you quit smoking,
and you no longer are stimulating your seretonin, you feel anxious and
irritable and you crave sweets.
Dr. Ferry: ... Except for tryptophan, which remains in the blood at high
levels
Dr. Ferry: Tryptophan is the building block to create seretonin.
Seretonin increases calmness and increases sugar cravings, so that's why you
crave sugar.
BarbChizmas_WebMD: What about weight gain? Do you gain more or less when
taking Zyban?
Dr. Ferry: Two large trials done from '95 to '98 have shown that during
a 7 to 9 week period after quitting smoking, people on Zyban gain less weight
than people who are on placebo. When you quit using Zyban, the effect on the
supposed appetite-center disappears in a matter of days, and craving or
increased appetite that remains after the disappearing of nicotine can lead to
excessive eating. People concerned about controlling their urges to eat and
cravings for sweets, may want to stay on Zyban for longer periods of time than
these two clinical trials were designed to demonstrate. This medication has
been used as an indication for depression, safely up to several years. So
there's no reason to be afraid to use it for a longer period of time than just
controlling the cravings for nicotine. Remember that nicotine suppresses a
normal appetite, therefore, most smokers but not all, have not dealt with a
healthy, normal adult appetite since they were adolescents. And learning to
handle and cope with that may exceed their coping strategies when food smells
better and tastes better after quitting smoking. The average weight gain when
people are not prepared for the increased appetite and craving is 5 to 7
pounds. But it is avoidable if someone understands the reasons why they smoke
and the 5 causes of weight gain after quitting.
In my book, How to Quit Smoking and Not Gain Weight, Mary Donkersloot and I
give a scientific basis for avoiding weight gain after discontinuing tobacco.
People gain weight for the following reasons. First, instead of the cigarette
in their fingers, and the hand to mouth action of smoking, they replace that
with food and eat in excess of 500 to 800 calories a day. #2, nicotine
withdrawal symptoms, as I explained earlier, can stimulate cravings for sweets
or food. #3, the nerve that creates the sense of smell in your nose, the
olfactory nerve, returns to normal functioning within 3 to 5 days after
discontinuing tobacco. The wonderful smell and taste of food can make otherwise
normal food seem more appealing to the recent ex-smoker and lead to overeating.
#4, smoking that delivers nicotine to the brain speeds up the body's metabolism
rate and burns calories faster. Quitting tobacco slows down the metabolic rate.
#5, smokers are often more sedentary than non-smokers and, therefore, do not
metabolize and utilize the normal calories eaten each day, and are therefore
more likely to gain weight after quitting smoking as adults. Nicotine does
suppress the normal appetite, which comes back to life within the first 1 to 2
weeks after discontinuing all nicotine products. This is a good thing and
should be celebrated when your appetite no longer is controlled under the
addicting influence of nicotine; just don't let it run away with you and learn
to control it.
Moderator: Are there no side effects to Zyban?
Dr. Ferry: Zyban is a medication that changes the chemistry in the human
brain. Anything that will change brain chemistry has its beneficial effects and
its potential detrimental effects. The side effects of Zyban are that a third
of people will also have chemical effects relating to two common symptoms. #1,
dry mouth in up to 38% of people. #2, difficulty sleeping. This is more common
in people who've used Zyban than in people who've quit smoking cold turkey.
Other uncommon symptoms of using Zyban are increase in headaches if people have
regular headaches prior to quitting smoking, upset stomach which can be
controlled by taking the medication with meals, constipation which can be
controlled by increasing the fiber in your diet and drinking 10 glasses or more
of water a day along with regular exercise. Feeling irritable or stimulated as
if drinking too much coffee; all of these side effects can be managed by
altering the dose of the medication or the timing of the medication. The dry
mouth and other symptoms may not change until your brain chemistry adjusts to
the effect of Zyban, about 2 to 3 weeks later. Very few of these side effects
are severe enough to discontinue the medication, as there are seldom deaths due
to dry mouth or insomnia but 400,000 people die every year because they don't
have the courage to stop smoking.
The one serious side-effect doctors should screen for is increased risk for
seizures; the 3 indicators to put someone at high risk, is having a family
history of seizures, a severe injury to your brain (gun shot wound, or skull
fracture), another concern is people who have a history of stroke, and those
who are currently abusing alcohol or other stimulant drugs. If those conditions
do not apply to the smoker, there is an extremely low rate of the risk of
seizures approximating less than 1 in 10,000 people. And we know 1 in 2 people
who continue to smoke will die of a tobacco related disease prematurely. So the
risk and benefit is entirely on the side of getting professional help to
determine the benefit of Zyban in your effort to quit smoking.
Moderator: What is "the patch" and how does it work?
Dr. Ferry: When someone says they've used the patch to quit smoking,
what they've done is delivered nicotine through something that looks like a
large circle or square band aid, in which nicotine is embedded in the adhesive.
Nicotine goes through the skin into the blood, travels back to the blood
through the lungs, and then to the brain. The smoker can't tell whether the
nicotine came from a lit cigarette or from the patch. The brain just recognizes
that nicotine is circulating and decreases nicotine withdrawal symptoms. Using
NRT, or gun, or nasal spray, or the oral inhaler of delivering nicotine into
the blood... that quit rate can be doubled to 10% and maybe 15% of all people.
This is according to large clinical trials. However, comparing that between men
versus women, there's a significant difference in most large studies showing
that men respond more favorably to the NRT, than women do. The evidence isn't
clear as to why men have a better respond to NRT. There is the suggestion that
men and women often smoke for different reasons; because of the woman's
hormonal makeup, estrogen and progesterone cycling every month, they may absorb
nicotine differently than men. This seems to be evident by that women use a
less number of cigarettes a day than men do, and nicotine levels in blood are
lower. That means a woman's brain gets the same effect with a lower dosage of
nicotine. Another concern is that men seem to smoke for reasons of aggression,
and to control nicotine withdrawal symptoms and anger, whereas women appear to
use tobacco to control their moods and emotions and stress. We know that twice
as many women are depressed over a lifetime, and we also know that the use of
tobacco changes the chemistry in a smoker's brain to decrease symptoms of
depression. Therefore, a lot of research is going on now to understand if women
are self-medicating undiagnosed depressive disorders, and when you just give
NRT, you don't really give what a woman wants from smoking. However, very
interesting news is that in the large trials done on Zyban, there's no
difference between the effectiveness on men versus women. Women quit at an
equally high rate than men do using this medicine. I believe we need to look
more closely into the question of whether Zyban is satisfying a primary reason
why a woman smokes compared to a man; that is, helping them deal with depressed
mood disorders so that they no longer need nicotine or tobacco to do that.
Moderator: How effective are some of these medications when taken in
combination?
Dr. Ferry: A large study of 900 patients compared Zyban and NRT alone
and in combination; the patients who quit smoking on Zyban alone were 36% at
the end of treatment, compared to NRT which was 23%. When you combined both
together, it was 39%. Looking at those results at 1 year, the Zyban therapy was
30%. NRT alone was 15%. When used in combination 35.5%. There are some people
that may benefit from using both together; its not clear exactly who those
people might be. Not everybody has a significant jump in success rates by
combining NRT with Zyban. But it is clear from this one study that Zyban is
more effective in the general smoking population than NRT alone. In fact, at 1
year, there was no difference from the placebo patients (who had received no
medication) and the NRT subjects, whereas, the Zyban patients had a
significantly higher, nearly double, the quit rate. I believe that patients
with the following conditions should talk to their physicians about combined
therapy: those who are very heavy smokers (2 to 3 packs a day), smokers with a
previous history of other chemical dependencies, and those with a previous
history of depression or other psychiatric illnesses. However, that's based on
10 years of clinical experience and not on clinical trials, as there have never
been any studies of the use of Zyban in patients with psychiatric illness.
Paninas_WebMD: Is there something, in addition to Zyban, that will curb
craving?
Dr. Ferry: There are several reasons for craving when someone is
abstaining from the use of tobacco; in order to extinguish all sources of
craving, you would have to live in an entirely sterile environment that would
have no cues or reminders of smoking behaviors. Therefore, its impossible for
an ex-smoker to say "Oh, I've never even had one craving." For
example, visual cues when someone isn't thinking of smoking can stimulate the
brain's chemistry, making someone desire tobacco. Visual cues are the most
difficult to distinguish. The smell of tobacco products again, even when you're
not thinking of smoking, can set off the trigger to desire use of tobacco and
set off cravings. #3, familiar environments where one naturally would reach for
a cigarette, or stressful situations like working on the computer or having an
argument with a boss or friend, or even if your brain wasn't prepared to have a
nicotine craving, can set off that chemical reaction. #4, the final method for
nicotine craving is the actual chemistry of the reward center in your brain;
this is the only source of craving that is modified by medications. Therefore,
medications will never eliminate all cues and triggers to smoke. Most of the
tips helping people to prepare to quit distinguishes the behaviors, thought
patterns, attitudes, and environments that help to eliminate a lot of the
unnecessary stimuli to crave tobacco. These are all essential to change prior
to someone quitting. Finally, understanding why you smoke by taking the quiz
"Why Do You Smoke?" can help you identify what your reasons are for
needing to smoke. If you can understand what your reasons are and meet those
needs by something other than tobacco that's satisfying, then you'll have less
craving and desire to smoke. The easy answer you may have been looking for
isn't some "natural" way to avoid craving besides taking NRT or
Zyban. We don't know of any other product that actually satisfies that part of
the brain and extinguishes that every 20 to 40 minute cycle that the brain
chemistry goes through needing another hit of tobacco, except that those
medications that work in the way nicotine does. There are many claims for
herbal products, but look carefully at their ingredients. They either have
caffeine or other stimulant products that work similarly to nicotine, but
they've never been proven to be effective... so it's probably not a good value
for dollar on your investment.
Moderator: How important is it to maintain a daily routine after
quitting smoking?
Dr. Ferry: My motto is that "preparation is everything".
Quitting is the simple part; people can quit a thousand times, but if you
aren't prepared to stay quit, it's a waste of effort. In order to prepare to
quit smoking, I recommend you establish an entirely new routine for your life
in the 1 to 4 weeks before your quit date, bringing into your rituals and
routines things that aren't associated with smoking. If you always sit down
with the same coffee mug in the same chair where you always smoke, what do you
expect your brain to do except to want to light up? My recommendation is that
you totally disrupt your comfortable, pleasant environment and situations that
you smoke prior to your quit date, and establish new habits and routines. Drink
milk instead of coffee. Drink tea or water. But don't go back to that familiar
coffee mug; throw it out and get a new one that won't be associated with the
visual cues to smoke. Buy a coffee mug that tells you not to smoke, and create
new rituals and patterns. If one of your patterns is coping styles to deal with
stress, then practice coping styles now for 5 to 10 minutes. And practice this
new behavior, so that it's comfortable and familiar when you finally do give up
your tobacco. A very important pattern to support a successful quit attempt is
regular meals, healthy snacking, daily exercise for the 2 weeks after you quit
smoking, and going to bed earlier than you normally would because nicotine
withdrawal sets up changes in your metabolic rates and sleep patterns in your
brain. You need that extra hour or two of sleep and exercise to re-establish
the brain chemistry that you want to be stabilized at after you quit using
nicotine. Another tip is to drink plenty of water; 6 to 8 glasses might be
adequate for someone small in stature, 8 to 10 glasses for someone who is large
frame or very tall. Nicotine is water-soluble; after your quit date, drinking
water eliminates nicotine quickly from your system, and the very active
drinking water stimulates dopamine release in your brain, stabilizing that
chemistry that creates the sense of pleasure and satisfaction. So yes, routines
are important to establish with new environments, not smoking in your car, and
establishing regular routines of not smoking to change your attitude prior to
your quit date. And that makes the transition much easier.
Moderator: What kinds of diets should someone that is quitting smoking
use, and which kinds should they stay away from?
Dr. Ferry: Because of the unstable chemical reactions that go on when
you're trying to get your brain off nicotine, it would not be in one's best
interest to also have highs and then lows from high sugar content which create
additional irritability, compounding nicotine withdrawal. My co-author, Mary
Donkersloot RD, and I believe that diets are counter-productive. Healthy
balanced nutrition is really the key to good health after quitting smoking. In
our book, we recommend a specific calorie amount and balance of carbohydrates,
proteins and fats for those first 24 hours after you quit smoking, and a
guideline for the whole first week after you quit smoking. The key is, when you
need something to replace the pleasure... use a fruit that you enjoy in the
most natural state as possible. Eat the whole apple with peel rather than drink
apple juice. Don't overdo it on high fat, high salt, or high sugar snack foods.
And be moderate in your portion sizes. Our book actually has in the second
half, a wide range of very healthy recipes for smokers to practice prior to
their quit date and to put into their regular routines, which gives high fiber,
reasonable protein levels, and complex carbohydrate balanced meals and recipes.
If you just eat every three to five hours with a small portion of a balanced
protein, carbohydrate and fat snack, rather than overeating because you are
depriving yourself and then get overly hungry, then you''ll find much more
stability in your eating patterns, your cravings, and weight gain. A variety of
examples are included in our book.
You see a cover of our book and the link to order it on my website -- The
Foundation For Innovations In Nicotine Dependence (www.findhelp.com). Or the
book can be ordered under the health and smoking cessations sections of
bookstores -- the authors are Mary Donkersloot and Linda Hyder-Ferry. The title
is How To Quit Smoking And Not Gain Weight Cookbook by Random House Publishers.
Moderator: Are there future drugs or treatments for quitting smoking and
what research is there?
Dr. Ferry: Some researchers are looking at the effectiveness of giving a
vaccine that blocks the transmission of nicotine from the blood to brain. And
we're not sure you could just overcome it by smoking more and longer. Other
medications similar to Zyban are being studied now that may work more
effectively on certain centers of the brain to target the pleasure and reward
centers with even less side effects than Zyban has. An important thing to
remember is that if you have an underlying depression or anxiety, ask your doctor
to screen you for those symptoms and to treat you prior to quitting smoking.
Many physicians don't realize that those underlying mood disorders can sabotage
a person's efforts to quit smoking, even when they're serious and trying very
hard to quit. Please don't be discouraged if you've tried to quit and it
failed; understand why you smoke and take that quiz on my website --
www.findhelp.com. Find alternative methods to meet your needs that don't
require tobacco, and move on to your smoke-free future.
Moderator: Is it helpful to quit smoking with a friend?
Dr. Ferry: We know that social support and befriending is important in a
variety of treatments for mental illness and addictive disorders. The most
successful method to quit the use of alcohol is Alcoholics Anonymous by
providing a social support system where people used to resort to alcohol. If
you are planning to quit smoking, you don't have to do it at the same time as
someone else, but you can get the support of someone who's also quitting and
can understand what you're going through and will be there for you. So buddy up
and let people know you're quitting, tell them your date, and make yourself
accountable to someone who loves you enough and helps you to quit. Checking in
with them on a daily basis is an excellent insurance policy for relapse
prevention.
Moderator: Thank you very much for joining us, Dr. Ferry. Please join us
every Wednesday at 9 pm EST here in the Mind and Body Auditorium for our live
weekly event. Next week we will be discussing The Psychological Impact of
Cancer and Its Treatments, with Dr. Anne Coscarelli.
Cigars: A Dangerous Habit
By Carlos Iribarren , MD, MPH, PhD
A lot of people think cigar smoking isn't dangerous because most cigar smokers
don't inhale. In fact, surveys suggest that about 10% of cigar aficionados do
inhale. But even those who don't purposely inhale still breathe in plenty of
second-hand smoke from a burning cigar -- and so do the people around them.
What's more, cigar smokers can't help swallowing some of the toxic substances
in cigar smoke, which contains greater concentrations of nicotine, benzene,
lead nitrogen oxides, and other nasty chemicals than does the smoke from
cigarettes. You should also know that cigar smoke generally has a higher pH (a
measure of acidity) than cigarette smoke. The higher pH facilitates the
absorption of nicotine through the lining of your mouth and nose, according to
research published in the Journal of the American Medical Association on
December 18, 1996.
Cigars may seem to carry less risk because most cigar smokers don't smoke as
often or as much as cigarette smokers. Yet in a study I recently co-authored
with several colleagues comparing cigar smokers with nonsmokers (The New
England Journal of Medicine, June 10, 1999), we found higher risks of heart
disease, chronic obstructive pulmonary disease, and cancers of the mouth,
esophagus, and lungs among men who puffed fewer than five cigars a day. As for
people who smoked more than five cigars a day, the risks went straight through
the roof -- tripling in the case of lung cancer. Interestingly, we also found
that the combination of drinking alcohol and smoking cigars raised the danger
even higher.
Our study was published at a time when sales of cigars had surged 50% in a
period of just five years, according to statistics from the U.S. Department of
Agriculture. Luckily, their popularity now appears to be leveling off and
perhaps even declining.
Don't fool yourself into thinking that it's safe to jump from that window on
the fourth floor. It's still a long way down. You'll do yourself a big favor by
jumping on another trend instead: kicking the cigar habit for good.
Want Better Sex?
Then put out that cigarette. Researchers are finding that smoking decreases both
desire and performance.
By Glenn Gordon
Mark Jordan, a 22-year-old substitute teacher in Phoenix, Ariz., had been
smoking for a year when the fire seemed to go out of his love life. "Sex
was suddenly getting boring," he says. "I didn't want to have it. I
would get out of breath so easily and I simply felt gross." While he
averaged only half a pack a day, on a weekend night he might smoke much more.
"I remember having sex in the shower and feeling like I was going to pass
out," he says. That was a turning point. He stopped smoking, started
exercising and eating right, and now says he has a much greater interest in sex
and enjoys it more than ever.
Watching Sharon Stone puff away in the film Basic Instinct may be stimulating
for some men, but smoking can be a major drag in a real-life bedroom (or
shower, as Jordan found). "Smoking has a direct, negative effect on the
sexuality of a man on every level," says Panayiotis M. Zavos, PhD,
director of the Andrology Institute of America and professor of reproductive
physiology and andrology at the University of Kentucky in Lexington.
Zavos and his fellow researchers studied 290 couples undergoing evaluation for
infertility and reported their results at the joint annual meeting the American
Society for Reproductive Medicine and the Canadian Fertility and Andrology
Society last September. As part of the study, couples completed a questionnaire
detailing their smoking and sexual habits. None of the women were currently
smoking, but 158 of the men, all between the ages of 26 and 35, smoked an
average of 30 cigarettes a day and had been smokers for an average of more than
seven years.
Lighting Up May Not Light Your Fire
Zavos' findings confirmed that men's smoking had a significant and negative
effect on a couples' ability to conceive. But they also turned up a surprise:
Smoking significantly diminished a man's sexual desire and satisfaction -- even
for young men in their 20s and 30s.
The smokers reported having sex less than six times a month whereas the nonsmoking
men were having sex nearly twice as often. This difference is especially
significant considering that these couples were actively trying to conceive.
"In current research, we are trying to identify how and why tobacco use
negatively impacts men's sexual performance. In my clinical experience, it does
decrease performance. Sexual performance is more than just erectile function,
it involves many of the systems of the body," says Zavos. "But when a
man's ability to have sex decreases, his appetite for sex will generally
follow."
Zavos found that when diminished desire is combined with impaired performance,
overall satisfaction is likely to suffer. When asked to rate their satisfaction
with the sex they were having on a scale of 1 to 10, nonsmoking couples
averaged 8.7, while couples with male smokers fared far worse with an average
of only 5.2. "There's no doubt in my mind," says Zavos, "that
nearly any man's sexual satisfaction and frequency [of having sex] would
increase if he stopped smoking."
Other experts agree that smoking can impair sexual performance. "Smoking
causes damage to smooth muscle inside the penis that interferes with erectile
functioning," says Richard Milsten, MD, co-author of The Sexual Male and a
urologist for more than 30 years in Woodbury, N.J. "So if men can't
perform as well, it would make sense that their libidos would suffer."
However, Milsten cautions against simple explanations for sexual behavior.
"There are so many factors in sexuality. Smoking is just one. Still, I
don't think it's outlandish to say that refraining from smoking will benefit
your sex life."
For Some Men, Cigarettes Still Seem Sexy
Larry Bullock, 36, an actor and model living in New York, has recently
considered breaking the habit. Bullock started smoking at 14 because it seemed
"masculine, adult, and cool." He says he has always enjoyed a very
high libido and never noticed any negative effects from smoking -- until
recently. "In fact, I loved smoking before and after sex," says
Bullock. "They were the best cigarettes of the day."
But lately, says Bullock, who will appear on the cover of an upcoming fitness
magazine, he began to notice that he was "feeling a bit winded"
during sex. "I get so out of breath and wheezy sometimes, that I've had to
ask my partner to refrain from asking me if I'm OK after orgasm."
What if you smoke fewer cigarettes or have been smoking for fewer years than
Bullock or the men in the survey? While Zavos admits to not having all the
answers, he speculates that whether or not you notice anything now,
"you're on a dangerous path."
Not everyone is convinced that smoke-free living will give them a new lease on
their sex life, however. "I quit for a few months," says Mathew
Lenning, a 25-year-old graphic designer in New York, who's been smoking since
high school, "but the only change I noticed about sex was that I really
missed having a cigarette afterwards."
Glenn Michael Gordon is a senior producer at iStash.com. He has written for YM,
Twist, Child, and Time Out New York magazines.
Panic Attacks More Common in Smokers
Mental Disorder Linked to Cigarettes
By Daniel J. DeNoon and Liz Meszaros
WebMD Medical News
If you think smoking calms you down, think again. A study of thousands of
smokers shows that they are three times more likely than nonsmokers to have
panic attacks and panic disorder.
"We know already a whole lot about the effects of smoking on just physical
health, and now we are also starting to see the adverse effects in new research
on mental illness," study co-author Naomi Breslau, PhD, tells WebMD.
"This is one example."
A panic attack can have all sorts of symptoms: shortness of breath, dizziness,
heart palpitations, trembling, sweating, choking, nausea, numbness, flushes or
chills, loss of one's sense of reality, chest pain, fear of dying, and/or fear
of going crazy. People who have frequent panic attacks (more than four in a
month) or have persistent fear of having another attack for a month after an
attack suffer from panic disorder.
Breslau says, "It's not simply that the two things go together, but it's
suggesting that smoking is playing a causal role." According to Breslau,
smoking increases a person's lifetime risk of a panic attack by three to four
times.
The risk of a first-time panic attack goes down in people who have quit
smoking, although the studies do not show whether quitting will eliminate all
risk in people who have smoked. But people who smoke should quit now, advises
Breslau, who is director of research in the psychiatry department of the Henry
Ford Health System. She and Donald F. Klein, MD, of the New York State
Psychiatric Institute published their findings in the December issue of the
journal Archives of General Psychiatry.
She suggested that tobacco smoke may induce panic attacks in susceptible
individuals. "There can be other mechanisms by which smoking induces
panic: the effect of nicotine for example," Breslau says. Nicotine has a
stimulating effect on the brain. It does all sorts of things."
Panic attacks may be a false alarm in which a person's body mistakenly thinks
it is suffocating, Klein previously has written. Based on this theory, Breslau
and Klein suggest in their article that carbon monoxide in cigarette smoke may
set off panic attacks in people predisposed to overreact.
In an interview seeking objective comment, clinical psychologist Benjamin
Fialkoff, PhD, tells WebMD that the study findings appear to be in line with
his experience in treating patients with panic disorder.
"It doesn't surprise me in view of the findings that smoking increases
stress," he said. "What we have in a panic response is the body's
stress response going full out. ... In general, you don't feel a soothing,
calming feeling after you have a cigarette."
Fialkoff says he prefers a combination treatment for patients with panic
disorder. He refers those patients willing to take medications to a physician
for a mild tranquilizer and an antidepressant. He then teaches patients ways to
reduce their anxiety symptoms, usually with breathing or relaxation techniques
but sometimes with self-hypnosis. When a specific irrational fear (phobia) is
involved, Fialkoff helps patients confront these fears in small, incremental
steps. Last but not least, he says he helps patients restructure their fearful
thoughts so that they do not lead to full-blown panic.
Vital Information:
- Smokers are three times more likely to have panic attacks -- and panic disorder -- than nonsmokers.
- In addition to harming a person's physical health, smoking can harm a person's mental health.
- Risk of panic attack gets smaller in people who quit smoking, but it is not clear how long it takes for the risk to go down.
Cigarette Makers Beat Back Secondhand Smoke Claim
By Michael Connor MIAMI (Reuters) - U.S. cigarette makers defeated the first
of about 3,200 individual secondhand smoke claims on Thursday, when a Miami
jury ruled the companies had no liability for the lung ailments of a former
flight attendant.
The six-person jury spent less than a day deciding against Marie Fontana, 59, a
former TWA flight attendant who relies on portable oxygen tanks and blamed her
sarcoidosis on passengers smoking on planes. "There is no liability for
the defendants," a Miami court official said. Philip Morris and other
cigarette makers paid $349 million in 1997 to settle a class-action suit on
behalf of flight attendants claiming injuries from secondhand smoke on U.S.
airliners. Smoking on U.S. domestic routes was banned in 1990.
But no plaintiff has yet received any cash, with $300 million set aside for a
health foundation and $49 million for plaintiffs' lawyers. The 1997 deal called
for follow-up trials on individual claims filed by last autumn. About 3,200
such claims are now in the pipeline, and Fontana's was the first to come to
trial.
Lawyers for the nonsmoking Fontana argued during a nearly three-week trial that
her sarcoidosis, a steadily worsening condition, and other lung ailments were
caused by passenger smoking on planes in the 1970s and 1980s.
Defense lawyers disputed that the secondhand smoke caused Fontana's sarcoidosis
and denied she had emphysema and chronic bronchitis as her lawyers said.
Fontana's lawyers, in asking for cash awards to cover lost wages and health
care costs, said she needs both of her lungs replaced and will require medical
care for the rest of her life. Lawyers said the Fontana case may prove crucial,
possibly affecting other anti-tobacco lawsuits throughout the United States.
The tobacco industry has been under courtroom and regulatory siege in the
United States since the mid 1990s.
Sanford C. Bernstein analyst Bill Pecoriello said in a research note issued
before the jury's decision that a favorable verdict for the defendants, such as
Philip Morris, the maker of Marlboros, and R.J. Reynolds Tobacco, would bode
well for the industry in the other flight attendants' cases awaiting trial.
Brown & Williamson, a unit of British American Tobacco Plc, and Lorillard,
a unit of Loews Corp, were also defendants in the Fontana suit.
Minutes After Smoking Cessation
Did you know that your body starts to show signs of being
healthier only 20 minutes after your last cigarette? By
that time, your blood pressure, pulse rate, and body
temperature all return to baseline levels. Of course, the
longer you stay tobacco-free, the healthier your body
becomes.
Quitting Smoking and Self-Efficacy
The role self-efficacy plays in behavior has been a considered to be an
important variable for many years. Recently, Jean-Francois Bergman Etter, Max
Humair Manfred and Thomas Jean-Paul Perneger examined the predictive utility of
self-efficacy and quitting smoking cigarettes. Specifically, the authors
created and tested an assessment instrument designed to measure smoker's belief
in their own ability to quit smoking, called the Smoking Self-Efficacy
Questionnaire (SEQ-12), a 12-items scale. The results of their empirical study
involving 644 participants suggests the instrument can be broken down into two
subscales, feeling depressed and external stimuli. The SEQ-12 appears to have
excellent psychometeric properties ( internal consistency coefficients were .95
and .94 for each scale and test-retest reliability coefficients were .95 and
.93). At the 16 month follow-up, score on the SEQ-12 predicted smoking
cessation status for current smokers. In other words, folks who scores high on
the SEQ-12 (i.e. people who believed that they were able to quit smoking, had
lower levels of depression and were willing and able to avoid associating with
other smokers) were more likely to be ex-smokers 16 months later. The authors
recommend the use of the instrument in both research and clinical settings. For
more details, see the original article in the journal Addiction (vol 95), June
2000, page 901-913.
Smoking Increases Skin Cancer Risk
We are already aware of many of the deleterious effects of smoking on the body.
Here is another one to add to the
list. A study published in the January 2001 issue of the Journal of Clinical
Oncology reported that the more
cigarettes an individual smokes, the greater the chance that he or she will
develop squamous cell carcinoma, a type
of skin cancer. See your doctor to discuss ways that you can quit smoking.
- M. Ellman
Bromocripting and Cigarette Smoking
In a recent article in the research journal Addiction, authors Murry Jarvik, Nicholas Caskey, William Wirshing, Damian Madsen, Paula Iwamoto-Schaap, Julie Elins, Naomi Eisenberger, and Richard Olmstead investigated the role bromocriptine can play in the treatment of cigarette smoking. In an empirical study, the authors compared 20 heavy smokers aged 18 to 58 years old. Half of the participants received 1 of 2 doses of bromocriptine (2.50 mg, 3.75 mg) over 3 sessions. The other half of the participants received a placebo. The smoking behaviors of all subjects were monitored and recorded for 5 hours after treatment. The experimental group (the group which received the bromocriptine treatment) was significantly different from the control group. Specifically, the people who received the bromocriptine treatment smoked fewer numbers of cigarettes and took fewer puffs off of each cigarette. In addition, the experimental group also had significantly lower levels of plasma nicotine and cotinine, which in turn is interpreted to mean that they not only craved cigarettes less than the control group, they also experienced less reinforcement from the nicotine. Finally, the researchers also found significantly lower levels of depression and decreased vigor than the control group. This is good news for individuals interested in augmenting their smoking cessation program with pharmaceutical interventions. The original article by the authors is in volume 95(8) of the journal Addiction (2000) pages 1173 to 1183.
Although bromocriptine appears to be beneficial for quitting smoking cigarettes, don't mistake it for a wonder drug. Like all medications, it does have its share of side-effects. Some serious side effects have occurred have included strokes, seizures (convulsions), and heart attacks. Some deaths have also occurred. You should discuss with your doctor the good that this medicine will do as well as the risks of using it. In addition, medical journals recommend against consuming any alcohol while on bromocriptine.
The following link provides some information from Excite's medical information page regarding bromocriptine.
http://health.excite.com/content/asset/uspdi.202094
Couple Approaches to Smoking Cessation
Carleton Palmer, Donald Baucom, and
Colleen McBride have recently written an interesting chapter in the book The Psychology of Couples and Illness:
Theory, Research and Practice (2000) in which they discuss, as the title would suggest, a couples-based
approach to quitting smoking. Specifically, the authors look at the impact of a
partner on a smoking person's behavior and habit and generate several useful
suggestions to maximize the likelihood of successful cessation. The authors
begin their chapter with a review of the literature regarding two person groups
and quitting smoking, stating that having a partner who continues to smoke is a
significant threat to continued abstinence once a person has quit smoking. This
is actually congruent with addiction literature with other substances. Alcohol,
cocaine and marijuana research as well as most 12-step programs emphasize the
need to discontinue relationships with using friends and associations.
Cigarette smoking, however, introduces a unique twist on this time tested and
honored recommendation of breaking off relations with individuals who continue
to use substances. Specifically, imagine someone entering an alcohol
rehabilitation program. Let's say that after years of struggling and multiple
loses, a husband begins treatment and experiences success in the initial
stages, but his wife states that she intends to continue drinking alcohol,
having alcohol in the house and inviting / encouraging visiting friends to have
a drink as well. Your average person would understand that this situation is
likely to be problematic and may, in fact, result in the marital discord and
possibly divorce. Alcoholism is frequently viewed as a serious condition that
frequently requires changes in the family unit during the course of treatment.
Now take the same scenario and replace alcohol with cigarettes. The idea that
someone might end a long-term monogamous relationship simply because one of the
partners refuses to quit smoking can seem more trivial and less understandable.
Although may would argue that the principal is the same and therefore
termination the relationship may become necessary, the authors of Couple
Approaches to Smoking Cessation emphasize attempting to work within the
relationship to aid in quitting. They recommend both partners examine their
reasons to continue to smoke and to quit, including looking at the costs and
benefits of each choice. Even if both partners don't decide to quit (or don't
decide to quit at the same time), the authors make recommendations regarding
how the individuals interact.
For example, they recommend avoiding negative-coercive behaviors (i.e.
nagging at or punishing each other, or using 'reverse-psychology' by making
statements like "I knew you couldn't do it.") and instead emphasize supportive
behaviors, targeting high-risk couple routines and couples therapy to reduce
relationship stress and conflict. I felt the authors emphasis on improving
couple relations and encouraging couple-based interventions is an interesting
and timely suggestion that anyone who is quitting smoking and has a partner who
smokes (and is planning to quit or keep smoking) is recommended to review.
Book Title: The Psychology of Couples and Illness: Theory, Research and
Practice (2000),
American Psychological Association, Washington DC
Relapses...
Know that most relapses occur in the
first week after quitting, when
withdrawal symptoms are strongest and your body is still dependent on
nicotine. Be aware that this will be your hardest time, and use all
your
personal resources; willpower, family, friends, and the tips in this
booklet- to get you through this critical period successfully.
Know that most other relapses occur in the first week after quitting,
when
situational triggers, such as a particularly stressful event, occur
unexpectedly. These are the times when people reach for cigarettes
automatically, because they associate smoking with relaxing. This is
the
kind of situation that's hard to prepare yourself for until it happens,
so
it's especially important to recognize it if it does happen. Remember
that
smoking is a habit, but a habit you can break.
Realize that most successful ex-smokers quit for good only after
several
attempts. You may be one of those who can quit on your first try. But
if
you're not, don't give up. Try again.
Reframing Health Behavior Change with Behavioral Economics
Warren K. Bickel, Ed., and Rudy E. Vuchinich, Ed., have written an in-depth examination of factors influencing the wide spread use of tobacco and the difficulties of quitting smoking. Their work is presented in one section of the book, Behavioral Economics of Tobacco Smoking (published by Lawrence Erlbaum Associates, Inc., 2000) gives an overview of basic concepts of behavioral economics of tobacco smoking. Their work suggests that several elements negatively impact an individual's attempt at quitting smoking. Specifically, they report that the low social, behavioral and economic cost required to obtain nicotine reinforcement from smoking is the primary factor promoting smoking. Bickel and Vuchinish suggest that, since there continues to be minimal negative social consequences for tobacco use, the relatively low cost of tobacco and the ease at which cigarettes can be obtained, quitting smoking is an enormously difficult task beyond the pure addictive properties of nicotine.
Anti-smoking program didn't have an impact
WASHINGTON (AP) -- It was to be a
showcase, world class demonstration of how to persuade school children not to
smoke.
The $15 million program used the latest smoking prevention theories
from the best social scientists. From the third grade on, children attended
special classes and were meticulously instructed by trained teachers how to
resist tobacco use.
But after 14 years, experts declared Tuesday that the project failed.
More than a fourth of the former Washington state school children in the study
are now regular smokers, about the same rate as those who didn't receive the
special classes, according to a report in the Journal of the National Cancer
Institute.
"It simply didn't work," said Arthur V. Peterson Jr., the
project's lead researcher. "It was a surprise. It was a
disappointment."
Peterson, who heads a cancer prevention program at Fred Hutchinson
Cancer Research Center in Seattle, said researchers are now scrambling to find
new approaches for controlling tobacco use among the young.
"It is time for researchers to go back to the drawing board,"
said Peterson.
He said techniques that have worked in some areas include denying
youthful access to tobacco by raising taxes and controlling sales, and by
countering tobacco company advertising with a heavy, youth-oriented media
blitz.
The Fred Hutchinson Cancer Research Center study, involving 8,388
school children and 640 teachers in 40 school districts, was based on what is
called a "social influences" approach.
The experiment included classes designed to arm children with the
skills to ignore social pressures to smoke, to teach them about the dangers of
smoking and to provide a motivation to remain smoke-free throughout life. The
students were taught to resist advertising, peer persuasion and influences at
home.
Children were targeted during the critical tobacco decision years --
the time in life when smoking habits that may last a lifetime are adopted.
The study started in September 1984 and continued until September 1999,
with researchers following the progress of the test children as they grew
older.
"This study was carefully conceived and meticulously performed,
and it achieved a new standard of scientific rigor for prevention
research," said Richard Clayton, a University of Kentucky researcher.
Yet it failed.
Surveys of the students in the study found that 24.4 percent of the
girls and 26.3 percent of the boys were daily smokers by the 12th grade. That
rate of smoking is almost identical to that among students who did not
participate in the study, researchers found.
Study Links Smoking, Colon Cancer
By PAUL RECER, AP Science Writer
WASHINGTON (AP) - Smoking cigarettes for 20 years or more can increase by more than 40 percent the risk of dying of colorectal cancer, according to a study that blames tobacco use for nearly one in eight such deaths in the United States. A team of American Cancer Society researchers report Wednesday in the Journal of the National Cancer Institute that a study of 781,351 people over 14 years showed a strong statistical linkage between cigarettes and death from colon or rectal cancer.
"It is clear that cigarette smoking is associated with colorectal cancer mortality for both men and women," Ann Chao, a researcher with the American Cancer Society and first author of the study, said Tuesday. Chao said earlier lab studies showed that carcinogens in cigarette smoke may cause tumors in the colon and rectum and may damage the DNA in cells. The new study is the first to link cigarettes and colorectal cancer death among such a large number people followed for such a long period of time, she said.
Based on the study, Chao concluded that of the approximately 56,000 Americans who die annually of colorectal cancer, about 6,800 of the deaths, some 12 percent, are associated with cigarette smoking. Colorectal cancer is diagnosed in more than 780,000 people worldwide annually, according to the World Health Organization. There about 129,400 cases of colorectal cancer identified in the U.S. annually, according to 1999 figures from the American Cancer Society.
Cigarette smoking is identified by the Centers for Disease Control and Prevention as the cause of 160,000 deaths from eight kinds of cancer, but colorectal cancer is not included on that list as a disease linked to tobacco use, said Chao. Chao and her co-authors suggest in the study that colorectal cancer now should be classified as a "smoking-related cancer." Dr. Bernard Levin of the University of Texas M.D. Anderson Cancer Center in Houston said the study gives strong support for classifying colorectal cancer as a smoking-related illness.
"This study and others show that
there is a high risk (of colorectal cancer) after 20 years or more of exposure (smoking),"
he said.
Levin, the vice president for cancer prevention at M.D. Anderson, said
the new study shows a clear dose-related effect from smoking: The more one
smokes, the greater the risk of cancer. Smoking also has been linked to death
from heart and pulmonary disease. The CDC estimates that cigarette smoking
causes more than 400,000 premature deaths annually. In the research, Chao and
her colleagues found that 4,432 people in the study group died of colon or
rectal cancer over the 14-year period.
An analysis of the smoking habits of the 781,351 people in the study, said Chao, showed the risk of colorectal cancer death increased steeply among 20-year smokers. The risk of death from the disease, she said, was directly linked to the number of cigarettes smoked and to the number of years that a person smoked. For instance, people in the study who smoked more than 40 cigarettes a day were 54 percent more likely to die of the cancer than were those who never smoked. Smokers who have puffed for more than 60 years were 48 percent more likely to die of colorectal cancer than those who never smoked.
The age when smoking started also played a role, said Chao. People who started the habit before the age of 15 had a 47 percent greater risk of dying from colorectal cancer than did those who never smoked. Quitting cigarettes lowered the risk, but not until 20 years after quitting, when the risk became similar to that of those who never smoked.
Losing Your Voice
Back in 1968, Virginia Slims
cigarettes capitalized on the burgeoning women's movement with its "You've
Come a Long Way, Baby" ads, linking smoking with freedom and independence.
Not only did the slogan become a popular catch-phrase, it helped boost
cigarette sales-and paved the way for other cigarette companies to market
directly to women. Within six years after the ads first appeared, the number of
12-year-old girls who smoked increased 110 percent, according to research
published in the Journal of the American Medical Association. Virginia Slims
(which is owned by Philip Morris U.S.A.) must have been hoping for a similar
success in the fall of 1999 when the brand launched a $40 million advertising
campaign using the language of personal empowerment. Headlined "Find Your
Voice," the campaign showcased artfully photographed women of various
ethnic groups, with text that included such phrases as "In silence I see.
With wisdom I speak." But "Find Your Voice" found nothing but
trouble.
When the ads, featuring black, white, Asian, and Hispanic models,
started appearing in women's magazines, anti-smoking advocacy groups went on
the offensive. "It was outrageous how they targeted young minority women,
who traditionally haven't smoked as much as white women," says Matthew
Myers, president of the Campaign for Tobacco-Free Kids. "Philip Morris saw
a new market and went after this community with the focus of a laser
beam."
Soon, the National Coalition for Women Against Tobacco, an 11
-million-member collective founded by the American Medical Women's Association,
and other groups had mobilized a counter campaign. Enlisting former tobacco
model and current cancer sufferer Janet Sachman as a spokeswoman, the National
Coalition demanded an immediate end to what it saw as the tobacco industry's
"newest attempt at recruitment." This past summer, Philip Morris's
CEO told a Florida jury looking to award punitive damages in a class-action
lawsuit brought against the nation's four biggest tobacco companies that the
"Find Your Voice" line was "a mistake." (The admission came
following the CEO's deposition, when a lawyer asked if "Find Your
Voice" might be offensive to ex-smokers who were now victims of throat
cancer.) Explaining that it doesn't "want people to look at our
advertising and say that we're trying to do something wrong," Philip
Morris edited out the offensive phrase-and then decided to shelve the entire
campaign.
-Kathleen Renda
No More Free Smokes
Phoenix (AP) -- R.J. Reynolds has agreed to stop mailing
cigarette samples to nonsmokers nationwide. Arizona Attorney General Janet
Napolitano had demanded since November that the Winston-Salem, N.C.,-based
tobacco manufacturer stop the practice.
R.J. Reynolds has maintained it did nothing wrong because the samples
were sent only to people were sent only to people who signed up for assorted
promotions and had certified that they were over age 21.
But in a letter Thursday to Napolitano from Reynolds vice president and
deputy general counsel Guy M. Blynn, the manufacturer acknowledged that its
mailing system for dealing with adult smokers is "flawed" because it
allows unsolicited mail to be sent.
Effective immediately, the company said it would stop sending product
samples nationwide to people in the current program, but the company will allow
those on the mailing list to choose whether to stay on the list or be removed.
Nicotine Patch
Nicotine patches were introduced in 1992 amid much fanfare. Millions of dollars have been spent advertising the merits of this smoking-cessation method. Newspapers and magazines are sprinkled with ads promoting the patch. Fortunately, this is a case in which the product will likely live up to its billing!
Description
Most nicotine patches look like large round Band-Aids. They contain a small amount of nicotine embedded in a special material. This material is kept in close contact with the skin by an adhesive.
How It Works
The patch releases
nicotine, which is absorbed by the skin. The nicotine then enters the
bloodstream. The amount of nicotine absorbed from the patch is lower than that
provided by smoking a cigarette.
It has been known for a while that nicotine can penetrate intact skin.
Over the last decade, a few investigators have studied nicotine patches and
found that skin absorption of nicotine could decrease cigarette cravings. Soon
thereafter a patch was developed that could release small amounts of nicotine
over a twenty-four-hour period.
Effectiveness
There are many reports that
the nicotine patch reduces cigarette cravings, and recent findings have
demonstrated that it can improve success rates among smokers who want to quit.
A recent report in The New England Journal of Medicine studied the
safety and effectiveness of nicotine skin patches designed to release nicotine
into the smoker's body over a sixteen-hour period. Subjects were given patches
that were to be placed on the skin in the morning and taken off at night. Some
were given patches that did not contain nicotine. No special counseling program
accompanied this intervention.
The researchers found that the subjects given the real nicotine patches
were more successful in quitting. The success rate at six weeks was 53 percent
in the nicotine-patch group and 17 percent in the other. At the end of a year,
the success rate was 17 percent in the nicotine-patch group and 4 percent in
the other group. Symptoms of nicotine withdrawal tended to be less in the
nicotine-patch group.
Another study involved nine medical centers and 935 patients. At the
six-month mark, 1 in 4 subjects treated with the nicotine patch remained a
nonsmoker as compared with 1 in 9 subjects treated with a patch that contained
no nicotine.
These studies provide compelling scientific evidence that the patch is
an effective aid for smoking cessation. There are few other methods that have
undergone such screening by the medical community and have been found to be
beneficial.
How to Use the Patch
The patches come in various
strengths including 22, 21,15,14,11,10, 7, and 5 milligrams, depending on the manufacturer.
The size of the patch is proportional to the amount of nicotine in it.
Therefore, the 21-milligram patch is the largest and the 5-milligram patch is
the smallest.
The patches may be used in a variety of different programs. One
approach is to use a larger patch for six weeks and then move to smaller
patches for two weeks each. Some people use the larger patch for a longer time.
There is no magic way to tell when you are ready to switch to a smaller patch.
It is usually recommended that at six weeks you give a smaller patch a
try. If you have trouble with symptoms when you switch, then you can always
return to the larger patch. As with the nicotine gum, you should not use the
patch unless you have stopped smoking.
The importance of this warning is highlighted by the recent reports of
heart attacks in people who were wearing a patch and smoking. Although the
contribution of the double dose of nicotine to the heart attack cannot be
proven, there is concern among some physicians that the added nicotine played a
role.
How to Place the Patch
The patch is designed to be placed on any non-hairy, clean, dry area of the body. The exact location of the patch does not matter. You should avoid areas that are oily, dirty, hairy, or irritated in any way. Open the storage packet and remove the patch. Place the patch on your skin and bold it there for about ten seconds, until you are sure that it sticks well. The entire patch, including the edges, should be firmly attached. Once you have placed the patch, you should wash your hands, since if you get nicotine in your eyes or nose, it could cause burning, stinging, or redness. The patch should remain in place for twenty-four hours and then be discarded. (Discard the patches in a place that is safe from children and pets.) If you leave the patch on for longer than twenty-four hours, it can irritate your skin. The next patch should be placed in a different location. You should not use one particular skin location more than once a week.
Side Effects
In recent large studies of the nicotine patch, there have been very few reported side effects. The most common complaint has been mild itchiness that lasted for fifteen to thirty minutes after placing the patch on the skin.
Does it matter at what time of day you apply the patch?
The time of day is not important. The patch can be put on at any time of the day or night, and this time can vary. All that you need to do is take off the old one and put on the new one.
What if you leave the patch on for longer than twenty-four hours?
Don't worry. The recommendation that the patch not be worn for longer than twenty-four hours is based on the observation that it may cause skin irritation. There should not be any other ill effects. Just remove the patch when you can.
Can you take a shower if you're wearing the patch?
The patch was designed to get wet without losing adhesiveness or effectiveness. You can bathe, swim, or shower while wearing it.
What if the patch falls off?
The patch is designed to stick well. If it does fall off, however, simply replace it. It is a good idea to carry an extra patch with you just in case you need it.
Which patch should you use?
Four nicotine-releasing adhesive patches for the skin - Nicoderm, Habitrol, Prostep, and Nicotrol - have been approved for the relief of nicotine withdrawal symptoms. They are all excellent products. Nicoderm and Habitrol are available in strengths of 7, 14, and 21 milligrams per day. Prostep is available in 11 and 22 milligrams per day, and Nicotrol is available in 5, 10, and 15 milligrams per day.
Nicotrol is designed to be worn only during waking hours, while the other patches should be worn for twenty-four hours. Nicotrol claims this is an advantage, but there is no evidence that indicates this patch is better than the others. In fact, there are no published comparisons of these patches in any clinical trials. Nevertheless, there are claims by the pharmaceutical companies that there are important differences in these patches relating to blood levels of nicotine, rate of allergic reactions, and ease of opening the package. At this time, all of the patches should be considered equally effective. The prices are similar; they average three dollars a day. The bottom line is that they are all excellent products and there is currently no clear advantage' to using one over the others.
Which dose should you use?
Patches should usually be started at the strongest strength. For Nicoderm and Habitrol, you should start with 21 milligrams per day; for Prostep, the 22-milligram strength; and for Nicotrol, 15 milligrams. For smokers who weigh less than 100 pounds, smoke less than half a pack of cigarettes per day, or who have cardiovascular disease, it may be preferable to start with a lower dose.
Physicians and Nicotine Replacement
Physicians may not always be the best source of information about nicotine replacement. A recent survey of California physicians practicing general medicine revealed that many were misinformed about the use of nicotine gum, even though almost 90 percent had prescribed it within the last year. Almost half of these physicians believed that, even if their patients did not stop smoking, they should use the gum to cut down on cigarettes. In addition, contrary to recommendations from authorities on smoking cessation, one in four of the doctors thought that the gum should not be used for more than one month.
The message is that not all doctors are informed (or even interested) in smoking cessation. It is your responsibility to educate yourself. If you are ready to quit, find a physician who knows about the gum or is familiar with the patch and has experience prescribing it.
Source: Krumholz, H. M. & Phillips, R.H. (1993) No If's, And's or Butts; the Smoker's Guide to Quitting , New York, Avery Publishing Group Inc.
Good News for Women: Stop Smoking, Not Eating
Ruth Kava
American Council on Science and Health
Smokers who quit smoking typically
gain a modest amount of weight. This
weight gain seems to deter many women from attempting to quit, even though
the health benefits of smoking cessation far outweigh any negative
health
effects of weight gain. "Fear of weight gain is particularly cited
by
female smokers," notes Dr. Nancy Rigotti of the Harvard Medical
School in
an editorial, "some of whom, it seems, would prefer to be slender
young
corpses rather than plump women with long lives."
But one hypothesis suggests that those who exercise regularly while
they
are quitting smoking may substantially diminish associated weight gain
as
well as improve their chances of quitting. A study by Dr. B. H. Marcus
and
coworkers published in the latest (June 14) issue of the Archives of
Internal Medicine, assessed whether exercise does indeed enhance the
ability to quit smoking and to maintain an ex-smoker status, while
reducing the tendency toward weight gain.
A total of 281 healthy but inactive young to middle-aged women took
part
in the study. On average, the participants had smoked more than one
pack
of cigarettes per day for over 20 years. The women participated in
either
a behavioral smoking-cessation program alone (the control group), or in
the same program with the addition of three supervised sessions of
vigorous aerobic exercise per week (the exercise group). All
participants
stopped smoking after the fifth week of the 12-week-long program.
Compared with the control group, the exercisers were significantly more
successful at maintaining their abstinence from smoking both 3 and 12
months after the formal program ended. At the same time, exercisers
were
in better physical condition and had gained significantly less weight
than
the sedentary quitters (6.7 versus 11.8 pounds).
Most of the effect of exercise on weight control was seen during the
period in which the subjects participated in the exercise intervention,
and the authors noted that weight gain was delayed but not completely
prevented in this trial. They suggested that this was due to some
subjects' stopping regular exercise once the 12 week treatment program
ended, and to others' possibly reducing their exercise frequency or
intensity once exercise sessions were no longer supervised.
Beyond the direct effects of exercise on increasing metabolic rate and
calorie expenditure, Marcus and colleagues state that "exercise
may also
have advantages that complement existing treatments," "is
effective in
modulating depression," and "is a beneficial strategy for
managing
stress." Women smokers should take heart from these results --
they can
both quit smoking and eat at least some cake-as long as they keep moving!
American Council on Science and Health
Nicotine: Is It Addictive?
The answer to that question is an
undeniable and resounding YES. Former U.S. Surgeon General C. Everett Koop
compares nicotine's grip on its users to that of heroin. According to a study
performed at the Henry Ford Health Sciences Center in Detroit, about 90 percent
of smokers are persistent daily users and 10 percent are occasional users.
That's almost the exact, reverse of another bad habit, excessive drinking. Only
10 to 15 percent of people who drink become dependent, problem drinkers, while
most people use alcohol on an occasional basis.
What makes nicotine so addictive? Just 11 seconds after you take a puff
of a cigarette--within five heartbeats--nicotine reaches the brain, where it
attaches itself to certain receptors in a part of the brain called the limbic
system. This action releases chemicals called neurotransmitters that affect
cognition and alertness, as well as feelings of pleasure and satisfaction.
Nicotine also increases the brain's uptake of glucose, an energy nutrient.
Finally, nicotine slows down communication between certain parts of the brain,
which causes you to feel more relaxed. Nicotine also causes your heart rate and
blood pressure to rise, giving you a sense of stimulation and increased energy.
Now you can see why you crave nicotine: It helps you think faster, calm
down, and feel pleasure--all within 11 seconds. If you smoke a pack a day and
take 10 puffs from each cigarette, you stimulate your brain with nicotine 200
times a day. Unfortunately, though, you'll probably need more and more nicotine
to get the same effect because most people develop a nicotine tolerance.
And those are just the purely physiological aspects of cigarette
addiction. There's more, much more, to this habit than meets the lungs and
brain.
So If I Quit Now, Will I Live Longer?
Did you know that people who quit
smoking live longer than people who continue to smoke? After fifteen years off cigarettes,
the risk of death for ex-smokers returns to nearly the level of people who have
never smoked. Male smokers who quit between ages 35to 39 add an average of five
years to their lives. Female quitters in this age group add three years to
their lives. These are averages - for some people, it's a lot more years.
If you're thinking that the earlier facts (see previous updates to the
web page below) about lung disease don't apply to you, as your family has no
history of lung cancers, it's important to consider the following: it's a
surprisingly overlooked fact that even more people die from heart disease
associated with smoking than from smoking-related cancers. Inpatients with
diabetes, a condition which often leads to heart disease, smoking further increases
heart and stroke risks.
Tobacco use is also associated with other diabetic complications,
including nervous system damage (neuropathy) and blindness caused by damage to
the retinas of the eyes (retinopathy). Blindness due to age-related macular degerations
is also more common among diabetics and nondiabetics who smoke. So, if either
heart disease or diabetes is part of your family's medical history, the facts
about the dangers of smoking are just as applicable to you.
What If You're Already Sick?
What if you already have a smoking-related illness? You'll be glad to know that the benefits of quitting smoking also apply to people who are currently sick:
|
For people with... |
Quitting smoking... |
|
Heart Disease |
Reduces the risk of repeat heart attacks and death from heart disease by 50 percent or more. |
|
Peripheral Artery
Disease |
Improves ability to exercise and increases overall survival. |
|
Ulcers |
Reduces the risk of recurrence and improves short-term healing. |
|
Lung Cancer |
Favorably improves response to many types of anticancer treatments and reduce3s risk of recurrence of cancer. |
Source: Fisher, E. B. (1998). 7 Steps to a Smoke-Free Life. John Wiley & Sons, Inc. New York.
Smoking Facts:
- 70% of all smokers want to quit
- 419,000 Americans die from diseases caused by smoking every year
- $65,000,000,000 cost to U.S. in healthcare and lost productivity
- 34% of smokers attempt to quit each year
- Cigarette smoking can cause impotency
- Quitting cigarettes can be harder than quitting heroin or cocaine
- Women who smoke have a 50% higher risk of having a heart attack than male smokers
- Women smokers are twice as likely as male smokers to get lung cancer
- Lung cancer has surpassed breast cancer as leading killer of American women
- Cigarettes are the leading cause of fire fatalities
- 1 pack per day puts 1 quart of tobacco tar in lungs each year
- Lung cancer is the leading cause of all cancer deaths
- Smoking is the single largest cause of preventable sickness and death in the United States.
- Approximately 40 million Americans smoke cigarettes...25% of the adult population.
- 17% of teenagers smoke.
- 3,000 teens start smoking every day.
- Parents who smoke are much more likely to have children who smoke.
- Half of all people who have ever smoked have now quit.
- The prevalence of smoking is highest among adults aged 25-40 (30%) and lowest among those 65+ (13%).
- The state with the highest percentage of smokers is Nevada (30.5%), followed by Alaska (28.0%) and Kentucky (27.9%).
- The state with the lowest percentage of smokers is Utah (15.6%), followed by Nebraska (17.4%) and Montana (18.0%).
- Smoking accounts for at least 7% of all health care costs in the US, an estimated $50 billion dollars in 1993.
- The federal government and state governments pay for more than 43% of all smoking-related medical expenses.
- Tobacco kills more Americans (450,000) each year than alcohol, cocaine, crack, heroin, homicide, suicide, car accidents, fire and
- AIDS combined.
IRS rewards those who quit smoking
SOURCE - WASHINGTON (AP)
Smokers trying to kick the habit can
claim some costs as medical expenses on income tax returns under a decision by
the Internal Revenue Service that reverses a 20-year-old agency position.
Doctors involved in smoking cessation programs said the IRS ruling could have
broader ramifications by persuading providers of health benefits packages to
include such treatment in their coverage. "It's about time," said Dr.
Mike Eriksen, director of smoking and health at the federal Centers for Disease
Control in Atlanta. "There is no better preventative program than stopping
someone from smoking."
Citing Surgeon General reports since 1988 that nicotine is addictive and
smoking harms health, the IRS concluded that programs and prescription drugs
that help someone quit smoking are no different from efforts to treat
alcoholism or drug addiction -- both of which are tax deductible.
"What the research of the last decade has documented is that this
is one of the most powerful addictions that a person can succumb to," said
Dr. Michael Fiore, director of the Center for Tobacco Research and Prevention
at the University of Wisconsin. "It's not just some bad habit. It's a
dangerous, chronic disease." In revoking its 1979 position against the
deduction, the IRS agreed.
"A strong causal link exists between smoking and several
diseases," the agency said in its announcement. "Nicotine, a
substance common to all forms of tobacco, is a powerfully addictive drug."
Not every expense can be deducted. The law does not permit a taxpayer to claim
such non-prescription medications as nicotine patches or gum. Also, the total
in medical expenses -- smoking-related or otherwise -- must reach 7.5 percent
of a taxpayer's adjusted gross income in order to qualify as an itemized
deduction. But prescriptions, doctor bills or cessation programs offered by
hospitals or other treatment facilities could be deducted, so long as they are
not reimbursed by an employer or by insurance.
Eriksen said there are an increasing number of intensive programs
available, including some at drug treatment centers that have added nicotine
addiction. There are also more and more pharmaceutical options, he said.
"It's the right thing to do in terms of the dollar invested and
the dollar saved," he said.
Taxpayers who paid for a smoking cessation program in recent years
could file an amended return to claim those costs, particularly if they already
had enough medical expenses to qualify.
Other taxpayers should check past returns to figure if the smoking
expenses reached the 7.5 percent of adjusted gross income threshold.
Taxpayers can generally file an amended return for three years after
the due date of the original return using IRS Form 1040X.
Exercise Helps Smokers Quit
SOURCE: Chicago (AP)
Women who exercise vigorously while trying to quit smoking are twice
as likely to kick the habit than ex-smokers who don't work out regularly, a new
study finds. The report also offers good news to female smokers who fear that
giving up tobacco and nicotine will lead to weight gain. Researchers found that
women who worked out as they tried to quit gained only about haft the weight of
those who did not.
"I can't say that definitively this will help all people, but
given all of the other health benefits associated with regular exercise I would
certainly encourage people trying to quit smoking to talk to their physicians
about starting a program," said Bess Marcus, an associate professor of
psychiatry and human behavior at Brown University and the study's lead author.
The findings appear in the Archives of Internal Medicine. Researchers
at The Miriam Hospital in Providence, R.I., followed 281 healthy but sedentary
female smokers who attended a 2-week program to stop smoking. Haft of the women
participated in supervised workouts three times a week during the program While
the others did not.
Of the 134 women in the group who exercised regularly, 19.4 percent
kicked the habit for at least two months after their program ended while 10.2
percent of the 147 non-exercisers did the same. Three months ~later, the
comparison of those still smoke-free was 16.4 percent to 8.2 percent,
respectively, and 11.9 percent vs. 5.4 percent a year later. The women ranged
between ages 18 and 65 and had smoked routinely for at least a year.
"There seems to be a new drug every day to help you quit
smoking," Marcus said in a telephone interview Sunday. "But this
study suggests that there's a drug-free alternative to quitting smoking if
that's what you prefer."
SOURCE: American Cancer Society
Many changes occur in the body after quitting smoking. The following list represents some of the common positive benefits that take place after you stop smoking:
- In 20 minutes: blood pressure falls and the pulse rate returns to normal.
- In 24 hours: chance of a heart attack decreases.
- In 48 hours: taste and smell are enhanced.
- In 2 weeks to 3 months: blood circulation improves and lung function increases up to 30 percent.
- In one month to nine months: coughing, sinus congestion, fatigue an shortness of breath decrease. Lunch function continues to improve and overall energy increases.
- In one year: excess risk of heart disease is half that of a smoker.
- In five years: rate of lung cancer drops by almost half.
- 5 to 15 years: risk of stroke is reduced to that of a nonsmoker. Risk of cancer of the mouth and throat is half that of a smoker.
- 10 years: Rate of lung cancer is similar to non-smokers.
- 15 years: Risk of heat disease is the same as for a non-smoker.
The benefits of quitting for your health and well-being are numerous and significant. It's never to late to stop smoking!
SOURCE: No If's And's or Butts: The Smoker's Guide to Quitting by Harlan Krumholz, MD and Robert Phillips, PhD
What Exactly Happens During Nicotine Withdrawal?
Nicotine is a syndrome resulting from the abrupt cessation or reduction of the use of nicotine-containing substances that have been employed for a least a moderate duration and in moderate amounts (approximately at least 5 weeks).
Symptoms of nicotine withdrawal include: heart rate may slow, blood pressure may rise and other physiological and psychological reactions. In order to be medically diagnoses with nicotine withdrawal you must meet the following criteria:
- Daily use of nicotine for at least several weeks
- Abrupt cessation or reduction of nicotine followed within twenty-four hours by at least four of the following symptoms:
- craving for nicotine
- irritability, frustration or anger
- anxiety
- difficulty concentrating
- restlessness
- decreased heart rate
- increased appetite or weight gain
Commonly reported symptoms also include: depression, disrupted sleep, impatience, impaired work performance and increase enjoyment of sweets. Cigarette craving is the most commonly experience symptoms.
BUT REMEMBER, these symptoms don't last forever!
SOURCE: Good Housekeeping, May 1998:
Smokers have many options available to them to aid in quitting smoking with the use of pharmaceutical interventions. The following table presents findings regarding effectiveness, side effects and costs for 5 commonly used medications.
|
Drug Name: |
Bupropion Hydrochloride (Zyban) |
|
How it Works |
Smokers start taking the drug about 2 weeks before they plan to quit and for 7 to 12 weeks afterward. The drug eases withdrawal symptoms by acting on the same brain receptors affected by nicotine. |
|
Effectiveness |
After 1 month, 49 percent of users still aren't smoking. A preliminary study found that after 1 year, 23 percent of users had kicked the habit. |
|
Side Effects |
Dry mouth, constipation and insomnia. Smokers who are taking other antidepressants and those who have kidney problems, epilepsy, alcoholism or eating disorders should not use. |
|
Cost |
About $270 for a 12-week supply (insurance may cover). |
|
Best For |
Smokers who don't want to use nicotine methods, or those who become depressed after quitting. |
|
Drug Name: |
Nicotine Inhaler (Nicotrol Inhaler) |
|
How it Works |
Smokers suck in nicotine vapor, satisfying the familiar hand-to-mouth ritual. The chemical even delivers the sensation smokers get in the back of their throat. The during is absorbed within 15 to 30 minutes. |
|
Effectiveness |
After a year, 10 to 20 percent of users still aren't smoking. |
|
Side Effects |
Mild irritation of the throat or mouth; coughing. Smokers with a asthma, allergies and sinus conditions should check with their doctors before using. |
|
Cost |
About $180 to $360 for a 2 month supply (insurance may cover). |
|
Best For |
Smokers who miss the hand-to-mouth ritual of the habit. |
|
Drug Name: |
Nicotine nasal spray (Nicotrol NS) |
|
How it Works |
The smoker squirts it into her nostrils whenever she feels the urge to light up. The drug is absorbed within 5 minutes. |
|
Effectiveness |
After a year, 10 to 20 percent of users still aren't smoking. |
|
Side Effects |
Nose and throat irritation; upset stomach. Smokers with asthma and allergies should check with their doctors before using. |
|
Cost |
About $280 for a 2 month supply (insurance may cover) |
|
Best For |
Pack-a-day smokers who need to satisfy their nicotine cravings quickly. |
|
Drug Name: |
Nicotine patch (NicoDermCQ, Nicotrol; Habitrol and Prostep by prescription only). |
|
How it Works |
Placed on the arm, the patch delivers nicotine into the blood stream over a 24-hour period. |
|
Effectiveness |
After a year, 10 to 20 percent of users still aren't smoking. |
|
Side Effects |
Reports of nausea and light-headedness in those who smoke while wearing the patch. Also, sleep disturbances and skin irritation. |
|
Cost |
About $240 to $300 for a 2-month supply (insurance may cover). |
|
Best For |
Smokers who prefer a low-maintenance product. |
|
Drug Name: |
Nicotine Gum (Nicorette) |
|
How it Works |
The smoker chews until she feels a slight tingling or peppery taste. Then she places the product between her cheek and gum until the sensation is gone. Nicotine is released into the bloodstream within 20 to 40 minutes. |
|
Effectiveness |
After a year, 10 to 30 percent of users still aren't smoking. |
|
Side Effects |
Some complaints of unpleasant taste. Smokers with dental problems, such as denture or temporomandibular joint dysfunction can't use. |
|
Cost |
About $240 for a 2-month supply (insurance probably won't cover). |
|
Best For |
Smokers who need to satisfy an oral fix, but don't want to use the inhaler). |
It is important to remember that smoking has many behavioral components. Without addressing these components (i.e. counseling, group therapy, work-shops, self-help treatment plans, etc.) it is likely that medications alone with fail.
The patch/nicotine-blocker (a substance that inhibits the pleasurable effects of nicotine) is in the final testing phase at the FDA and may be on the market as soon as next year.